
Death and Dying

Learning Objectives
At the end of this chapter, you will be able to:
- Compare the leading causes of death in the United States with those of developing countries.
- Compare physiological, social, and psychic death.
- List and describe the stages of loss based on various models including that of Kubler-Ross.
- Explain the philosophy and practice of palliative care.
- Describe hospice care.
- Differentiate attitudes toward hospice care based on race and ethnicity.
- Compare euthanasia, passive-euthanasia, and physician-assisted suicide.
- Characterize bereavement and grief.
- Express your own ideas about death and dying.
Introduction
We have now reached the end of the lifespan. While it is true that death occurs more commonly at the later stages of age, death can occur at any point in the life cycle. Death is a deeply personal experience evoking many different reactions, emotions, and perceptions.
“Everything has to die,” he told her during a telephone conversation.
“I want you to know how much I have enjoyed being with you, having you as my friend, and confident and what a good father you have been to me. Thank you so much.” she told him.
“You are entirely welcome.” he replied.
He had known for years that smoking will eventually kill him. But he never expected that lung cancer would take his life so quickly or be so painful. A diagnosis in late summer was followed with radiation and chemotherapy during which time there were moments of hope interspersed with discussions about where his wife might want to live after his death and whether or not he would have a blood count adequate to let him proceed with his next treatment. Hope and despair exist side by side. After a few months, depression and quiet sadness preoccupied him although he was always willing to relieve others by reporting that he ‘felt a little better’ if they asked. He returned home in January after one of his many hospital stays and soon grew worse. Back in the hospital, he was told of possible treatment options to delay his death. He asked his family members what they wanted him to do and then announced that he wanted to go home. He was ready to die. He returned home. Sitting in his favorite chair and being fed his favorite food gave way to lying in the hospital bed in his room and rejecting all food. Eyes closed and no longer talking, he surprised everyone by joining in and singing “Happy birthday” to his wife, son, and daughter-in-law who all had birthdays close together. A pearl necklace he had purchased 2 months earlier in case he died before his wife’s birthday was retrieved and she told him how proud she would be as she wore it. He kissed her once and then again as she said goodbye. He died a few days later[1].
Except for a handful of illnesses in which death does often quickly follow diagnosis, or in the case of accidents or trauma, most deaths come after a lengthy period of chronic illness or frailty (Institute of Medicine (IOM), 2015).
A dying process that allows an individual to make choices about treatment, to say goodbyes and to take care of final arrangements is what many people hope for. Such a death might be considered a “good death.” But of course, many deaths do not occur in this way. While modern medicine and better living conditions have led to a rise in life expectancy around the world, death will still be the inevitable final chapter of our lives.
Not all deaths include such a dialogue with family members or being able to die in familiar surroundings. People die suddenly and alone. People leave home and never return. Children precede parents in death; wives precede husbands, and the homeless are bereaved by strangers. In this chapter, we look at death and dying, grief and bereavement. We explore palliative care and hospice. And we explore funeral rites and the right to die.
Defining Death
One way to understand death and dying is to look more closely at what defines physical death and social death.
Death Defined: According to the Uniform Determination of Death Act (UDDA) (Uniform Law Commissioners, 1980), death is defined clinically as the following: An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. A determination of death must be made in accordance with accepted medical standards.
The UDDA was approved for the United States in 1980 by a committee of national commissioners, the American Medical Association, the American Bar Association, and the President’s Commission on Medical Ethics. This act has since been adopted by most states and provides a comprehensive and medically factual basis for determining death in all situations.
Aspects of Death
One way to understand death and dying is to look more closely at physical death, psychological death, and social death. These deaths do not occur simultaneously. Rather, a person’s physiological, social, and psychic death can occur at different times[2].
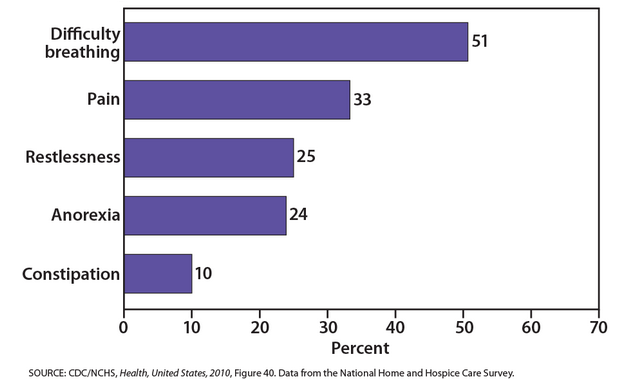
Physiological death occurs when the vital organs no longer function. The digestive and respiratory systems begin to shut down during the gradual process of dying. A dying person no longer wants to eat as digestion slows and the digestive tract loses moisture and chewing, swallowing, and elimination becomes painful processes. Circulation slows and mottling or the pooling of blood may be noticeable on the underside of the body appearing much like bruising. Breathing becomes more sporadic and shallower and may make a rattling sound as air travels through mucus filled passageways. The person often sleeps more and more and may talk less although continues to hear. The kinds of symptoms noted prior to death in patients under hospice care (care focused on helping patients die as comfortably as possible) are noted below. When a person no longer has brain activity, they are clinically dead. Physiological death may take 72 or fewer hours.
Social death begins much earlier than physiological death. Social death occurs when others begin to withdraw from someone who is terminally ill or has been diagnosed with a terminal illness. Those diagnosed with conditions such as AIDS or cancer may find that friends, family members, and even health care professionals begin to say less and visit less frequently. Meaningful discussions may be replaced with comments about the weather or other topics of light conversation. Doctors may spend less time with patients after their prognosis becomes poor. Why do others begin to withdraw? Friends and family members may feel that they do not know what to say or that they can offer no solutions to relieve suffering. They withdraw to protect themselves against feeling inadequate or from having to face the reality of death. Health professionals, trained to heal, may also feel inadequate and uncomfortable facing decline and death. A patient who is dying may be referred to as “circling the drain” meaning that they are approaching death. People in nursing homes may live as socially dead for years with no one visiting or calling. Social support is important for quality of life and those who experience social death are deprived of the benefits that come from loving interaction with others.
Psychic death occurs when the dying person begins to accept death and to withdraw from others and regress into the self. This can take place long before physiological death (or even social death if others are still supporting and visiting the dying person) and can even bring physiological death closer. People have some control over the timing of their death and can hold on until after important occasions or die quickly after having lost someone important to them. They can give up their will to live.
Death Process: For those individuals who are terminal and death is expected, a series of physical changes occur. Individual experiences may be influenced by such variables as the cause of death, the person’s general health, medications and other significant factors. All dying experiences are unique and influenced by many factors, such as the particular illness and the types of medications being taken, but there are some physical changes that are fairly common.
Bell (2010) identifies some of the major changes that occur in the weeks, days, and hours leading up to death:
Weeks Before Passing
o Minimal appetite; prefer easily digested foods
o Increase in the need for sleep
o Increased weakness
o Incontinence of bladder and/or bowel
o Restlessness or disorientation
o Increased need for assistance with care
Days Before Passing
o Decreased level of consciousness
o Pauses in breathing
o Decreased blood pressure
o Decreased urine volume and urine color darkens
o Murmuring to people others cannot see
o Reaching in air or picking at covers
o Need for assistance with all care
Days to Hours Before Passing
o Decreased level of consciousness or comatose-like state
o Inability to swallow
o Pauses in breathing become longer
o Shallow breaths
o Weak or absent pulse
o Knees, feet, and/or hands becoming cool or cold
o Knees, feet, and/or hand discoloring to a purplish hue
o Noisy breathing due to relaxed throat muscles often called a “death rattle”
o Skin coloring becoming pale, waxen (pp. 5, 176-177)
Most Common Causes of Death
The United States: In 1900, the most common causes of death were infectious diseases which brought death quickly. Today, the most common causes of death are chronic diseases in which a slow and steady decline in health ultimately results in death.
| Top 3 leading causes of death in the United States | |
| 1900’s | 1990’s |
| Pneumonia & Influenza | Heart Disease |
| Tuberculosis | Cancer |
| Diarrhea & Enteritis | Stroke |
| 30% of all deaths | 60% of all deaths. |
These were the top causes of death for various age groups in the United States in the year 2016 (CDC):
|
Age range |
Top cause of death |
|
< 1 year |
Congenital anomalies |
|
1 – 4 years |
Unintentional Injury |
|
5 – 9 years |
Unintentional Injury |
|
10 – 14 years |
Unintentional Injury |
|
15 – 24 years |
Unintentional Injury |
|
25 – 34 years |
Unintentional Injury |
|
35 – 44 years |
Unintentional Injury |
|
45 – 54 years |
Malignant Neoplasms (cancer) |
|
55 – 64 years |
Malignant Neoplasms (cancer) |
|
65 + |
Heart Disease |
How might cause of death the way we think of death, how we grieve, and the amount of control a person has over his or her own dying process?
|
|
American Asian |
White |
Black |
Pacific Islander |
Hispanic |
|
1 |
Heart Disease |
Heart Disease |
Heart Disease |
Heart Disease |
Heart Disease |
|
2 |
Cancer |
Cancer |
Cancer |
Cancer |
Cancer |
|
3 |
Stroke |
Stroke |
Diabetes |
Stroke |
Stroke |
|
4 |
COPD |
Diabetes |
Stroke |
Pneu/Influenza |
COPD |
|
5 |
Pneu/Influenza |
Pneu/Influenza |
COPD |
COPD |
Pneu/Influenza |
Deadliest Diseases Worldwide
The top 10 deadliest diseases in the world are listed below along with the estimated number of deaths per cause. These figures are for 2016 and do not reflect deaths due to violence or suicide (World Health Organization, World Health Report, 2018). Many of these deaths are due to preventable causes. Deaths due to neurocognitive disorders (dementias) more than doubled between 2000 and 2016, making it the 5th leading cause of global deaths in 2016 compared to 14th in 2000.
- Heart disease (9.4 million)
- Stroke (5.7 million)
- Chronic obstructive pulmonary disease COPD (3.0 million)
- HIV/AIDS (2.9 million)
- Alzheimer’s and other dementias (1.9 million)
- Trachea, Bronchus, and lung cancers (1.7 million)
- Diabetes mellitus (1.6 million)
- Road injury (1.4 million)
- Diarrhoeal diseases (1.4 million)
- Tuberculosis (1.3 million)
Developmental Perceptions of Death and Death Anxiety
The concept of death changes as we develop from early childhood to late adulthood. Cognitive development, societal beliefs, familial responsibilities, and personal experiences all shape an individual’s view of death.[4]

Infancy: Certainly, infants do not comprehend death, however, they do react to the separation caused by death. Infants separated from their mothers may become sluggish and quiet, no longer smile or coo, sleepless, and develop physical symptoms such as weight loss.
Early Childhood: As you recall from Piaget’s preoperational stage of cognitive development, young children experience difficulty distinguishing reality from fantasy. It is therefore not surprising that young children lack an understanding of death. They do not see death as permanent, assume it is temporary or reversible, think the person is sleeping, and believe they can wish the person back to life. Additionally, they feel they may have caused death through their actions, such as misbehavior, words, and feelings.
Middle Childhood: Although children in middle childhood begin to understand the finality of death, up until the age of 9 they may still participate in magical thinking and believe that through their thoughts they can bring someone back to life. They also may think that they could have prevented the death in some way, and consequently feel guilty and responsible for the death.
Late Childhood: At this stage, children understand the finality of death and know that everyone will die, including themselves. However, they may also think people die because of some wrongdoing on the part of the deceased. They may develop fears of their parents dying and continue to feel guilty if a loved one dies.
Adolescence: Adolescents understand death as well as adults. With formal operational thinking, adolescents can now think abstractly about death, philosophize about it, and ponder their own lack of existence. Some adolescents become fascinated with death and reflect on their own funeral by fantasizing on how others will feel and react. Despite a preoccupation with thoughts of death, the personal fable of adolescence causes them to feel immune to death. Consequently, they often engage in risky behaviors, such as substance use, unsafe sexual behavior, and reckless driving thinking they are invincible.
Early Adulthood: In adulthood, there are differences in the level of fear and anxiety concerning death experienced by those in different age groups. For those in early adulthood, their overall lower rate of death is a significant factor in their lower rates of death anxiety. Individuals in early adulthood typically expect a long life ahead of them, and consequently do not think about, nor worry about death.
Middle Adulthood: Those in middle adulthood report more fear of death than those in either early or late adulthood. The caretaking responsibilities for those in middle adulthood is a significant factor in their fears. As mentioned previously, middle adults often aid with both their children and parents and they feel anxiety about leaving them to care for themselves.
Late Adulthood: Contrary to the belief that because they are so close to death, they must fear death, those in late adulthood have lower fears of death than other adults. Why would this occur? First, older adults have fewer caregiving responsibilities and are not worried about leaving family members on their own. They also have had more time to complete activities they had planned in their lives, and they realize that the future will not provide as many opportunities for them. Additionally, they have less anxiety because they have already experienced the death of loved ones and have become accustomed to the likelihood of death. It is not death itself that concerns those in late adulthood; rather, it is having control over how they die.
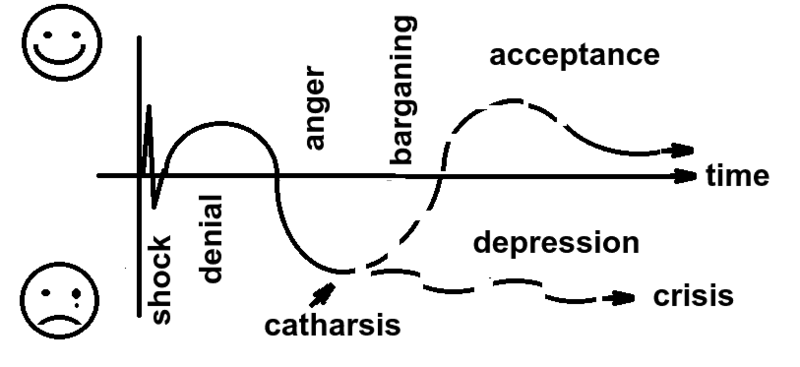
Five Stages of Loss
Kubler-Ross[5] describes five stages of loss experienced by someone who faces the news of their impending death. These “stages” are not really stages that a person goes through in order or only once; nor are they stages that occur with the same intensity. Indeed, the process of death is influenced by a person’s life experiences, the timing of their death in relation to life events, the predictability of their death based on health or illness, their belief system, and their assessment of the quality of their own life. Nevertheless, these stages help us to understand and recognize some of what a dying person experiences psychologically. And by understanding, we are more equipped to support that person as they die.
Denial is often the first reaction to overwhelming, unimaginable news. Denial, or disbelief or shock, protects us by allowing such news to enter slowly and to give us time to come to grips with what is taking place. The person who receives positive test results for life-threatening conditions may question the results, seek second opinions, or may simply feel a sense of disbelief psychologically even though they know that the results are true.
Anger also provides us with protection in that being angry energizes us to fight against something and gives structure to a situation that may be thrusting us into the unknown. It is much easier to be angry than to be sad or in pain or depressed. It helps us to temporarily believe that we have a sense of control over our future and to feel that we have at least expressed our rage about how unfair life can be. Anger can be focused on a person, a health care provider, at God, or at the world in general. And it can be expressed over issues that have nothing to do with our death; consequently, being in this stage of loss is not always obvious.
Bargaining involves trying to think of what could be done to turn the situation around. Living better, devoting yourself to a cause, being a better friend, parent, or spouse, are all agreements one might willingly commit to if doing so would lengthen life. Asking to just live long enough to witness a family event or finish a task are examples of bargaining.
Depression is sadness and sadness is appropriate for such an event. Feeling the full weight of loss, crying, and losing interest in the outside world is an important part of the process of dying. This depression makes others feel very uncomfortable and family members may try to console their loved one. Sometimes hospice care may include the use of antidepressants to reduce depression during this stage.
Acceptance involves learning how to carry on and to incorporate this aspect of the life span into daily existence. Reaching acceptance does not in any way imply that people who are dying are happy about it or content with it. It means that they are facing it and continuing to make arrangements and to say what they wish to say to others. Some terminally ill people find that they live life more fully than ever before after they come to this stage.
There is no “right way” to experience the loss. People move through a variety of stages with different frequency and in various ways. It is important to note that Kübler-Ross’s work may not apply to everyone who is grieving. Her research focused only on those who were terminally ill. Friedman and James (2008) and Telford et al. (2006) expressed concern that mental health professionals, along with the general public, may assume that grief follows a set pattern, which may create more harm than good. Lastly, the Yale Bereavement Study, completed between January 2000 and January 2003, did not find support for Kübler-Ross’s five-stage theory of grief [6]. Results indicated that acceptance was the most commonly reported reaction from the start, and yearning was the most common negative feature for the first 2 years. The other variables, such as disbelief, depression, and anger, were typically absent or minimal.
Palliative Care and Hospice
When individuals become ill, they need to make choices about the treatment they wish to receive. One’s age, type of illness, and personal beliefs about dying affect the type of treatment chosen (Bell, 2010).
Curative care is designed to overcome and cure disease and illness.[7] Its aim is to promote complete recovery, not just to reduce symptoms or pain. An example of curative care would be chemotherapy. While curing illness and disease is an important goal of medicine, it is not its only goal. As a result, some have criticized the curative model as ignoring the other goals of medicine, including preventing illness, restoring functional capacity, relieving suffering, and caring for those who cannot be cured.
Palliative care focuses on providing comfort and relief from physical and emotional pain to patients throughout their illness even while being treated (NIH, 2007). Palliative care is an interdisciplinary approach to specialized medical and nursing care for people with life-limiting illnesses. Although it is an important part of end-of-life care, it is not limited to that stage. Palliative care is provided by a team of physicians, nurses, physiotherapists, occupational therapists, speech-language pathologists, and other health professionals who work together with the primary care physician and referred specialists to provide additional support to the patient. It focuses on providing relief from the symptoms, pain, physical stress, and mental stress at any stage of illness, with a goal of improving the quality of life for both the person and their family. Medical staff who specialize in palliative care have training tailored to helping patients and their family members cope with the reality of the impending death and make plans for what will happen after.
Palliative care is part of hospice programs. Hospice involves caring for dying patients by helping them be as free from pain as possible, providing them with assistance to complete wills and other arrangements for their survivors, giving them social support through the psychological stages of loss, and helping family members cope with the dying process, grief, and bereavement. In order to enter hospice, a patient must be diagnosed as terminally ill with an anticipated death within 6 months. Most hospice care does not include medical treatment of disease or resuscitation although some programs administer curative care as well. The patient is allowed to go through the dying process without invasive treatments. Family members, who have agreed to put their loved one on hospice, may become anxious when the patient begins to experience the death. They may believe that feeding or breathing tubes will sustain life and want to change their decision. Hospice workers try to inform the family of what to expect and reassure them that much of what they see is a normal part of the dying process.
|
According to Shannon (2006), the basic elements of hospice include:
Bereavement counseling for the family up to one year after the patient’s death |
Today, there are more than 4,000 hospice programs and over 1,000 of them are offered through hospitals. In 2013, an estimated 1.5 million people received hospice care.[8]The majority of patients on hospice are cancer patients and typically do not enter hospice until the last few weeks prior to death. The majority of patients on hospice are cancer patients whotypically do not enter hospice until the last few weeks prior to death. The average length of stay is less than 30 days.[9] The median length of stay was 18 days, and one out of three patients were on hospice for less than a week. Although hospice care has become more widespread, these new programs are subjected to more rigorous insurance guidelines that dictate the types and amounts of medications used, length of stay, and types of patients who are eligible to receive hospice care.[10] Thus, more patients are being served, but providers have less control over the services they provide, and lengths of stay are more limited. Patients receive palliative care in hospitals and in their homes. When hospice is administered at home, family members may also be part, and sometimes the biggest part, of the care team. Certainly, being in familiar surroundings is preferable to dying in an unfamiliar place. But about 60 to 70% of people die in hospitals and another 16% die in institutions such as nursing homes.[11] Most hospice programs serve people over 65; few programs are available for terminally ill children.[12]

The Hospice Foundation of America notes that not all racial and ethnic groups feel the same way about hospice care. African-American families may believe that medical treatment should be pursued on behalf of an ill relative as long as possible and that only God can decide when a person dies. Chinese-American families may feel very uncomfortable discussing issues of death or being near the deceased family member’s body. The view that hospice care should always be used is not held by everyone and health care providers need to be sensitive to the wishes and beliefs of those they serve.[13]
Family Care
According to the Institute of Medicine [14], it is estimated that 66 million Americans, or 29% of the adult population, are caregivers for someone who is dying or chronically ill. Two-thirds of these caregivers are women. This care takes its toll physically, emotionally, and financially. Family caregivers may face the physical challenges of lifting, dressing, feeding, bathing, and transporting a dying or ill family member. They may worry about whether they are performing all tasks safely and properly, as they receive little training or guidance. Such caregiving tasks may also interfere with their ability to take care of themselves and meet other family and workplace obligations. Financially, families may face high out of pocket expenses.[15], most family caregivers are employed, are providing care by themselves with little professional intervention, and there are high costs in lost productivity. As the prevalence of chronic disease rises, the need for family caregivers is growing. Unfortunately, the number of potential family caregivers is declining as the large baby boomer generation enters into late adulthood.[16]
|
Characteristic |
|
|
No home visits by health care professionals |
69% |
|
Caregivers are also employed |
72% |
|
Caregivers for the elderly |
67% |
|
% of employed workers who have been caregiving for 3+ years |
55% |
End of Life Decisions
Advanced Directives
Advanced care planning refers to all documents that pertain to end-of-life care. These include advance directives and medical orders. Advance directives include documents that mention a healthcare agent and living wills. These are initiated by the patient. Living wills are written or video statements that outline the health care initiate the person wishes under certain circumstances. A durable power of attorney for healthcare names the person who should make healthcare decisions in the event that the patient is incapacitated. In contrast, medical orders are crafted by a medical professional on behalf of a seriously ill patient. Unlike advanced directives, as these are doctor’s orders, they must be followed by other medical personnel. Medical orders include Physician Orders for Life-sustaining Treatment (POLST), do-not-resuscitate, do not-incubate or do-not-hospitalize. In some instances, medical orders may be limited to the facility in which they were written. Several states have endorsed POLST so that they are applicable across healthcare settings.[18].
Despite the fact that many Americans worry about the financial burden of end-of-life care, “more than one-quarter of all adults, including those aged 75 and older, have given little or no thought to their end-of-life wishes, and even fewer have captured those wishes in writing or through conversation” [19]
Euthanasia
Euthanasia, or helping a person fulfill their wish to die, can happen in two ways: voluntary euthanasia and physician-assisted suicide. Voluntary euthanasia refers to helping someone fulfill their wish to die by acting in such a way to help that person’s life end. Euthanasia can be by passive euthanasia such as no longer feeding someone or giving them food. Or it can be active euthanasia such as administering a lethal dose of medication to someone who wishes to die.
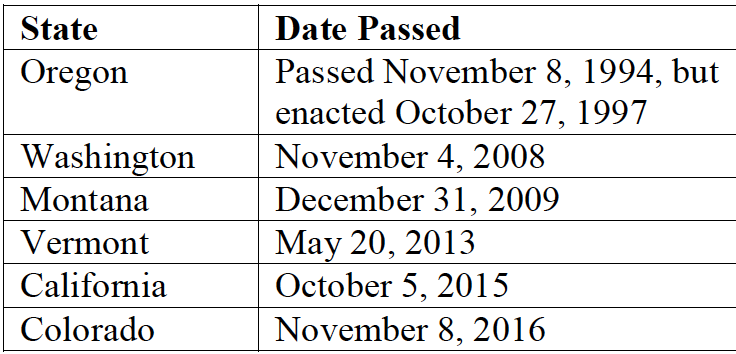
Physician-assisted suicide involves active euthanasia and occurs when a physician prescribes the means by which a person can end his or her own life. Physician-assisted suicide is legal in six states in the U.S., Canada, the Netherlands, Luxembourg, Switzerland, and Belgium. The person seeking physician-assisted suicide for US states must be: (1) at least 18 years of age, (2) have six or less months until expected death, and (3) obtain two oral (or least 15 days apart) and one writtenrequest from a physician (ProCon.org, 2016). In 2014, Belgium allows the right to die to those under the age of 18. Stricter conditions were put in place for children, including parental consent, the child must be suffering from a serious and incurable disease, the child must understand what euthanasia means, and the child’s death must be expected in the near future (Narayan, 2016). Physician-assisted suicides, however, are rare. Since 1997 when the law was passed in Oregon, 1545 people had lethal prescriptions written and 991 patients had died from the medication by the end of 2015.[20]
The practice of physician-assisted euthanasia is certainly controversial with religious, legal, ethical, and medical experts weighing in with opinions. The main areas where there is disagreement between those who support physician-assisted euthanasia and those who do not include: (1) whether a person has the legal right to die, (2) whether active euthanasia would become a “slippery slope” and start a trend to legalize deaths for individuals who may be disabled or unable to give consent, (3) how to interpret the Hippocratic Oath and what it exactly means for physicians to do no harm, (4) whether the government should be involved in end-of-life decisions, and (5) specific religious restrictions against deliberately ending a life (ProCon.org, 2016). Not surprisingly, there are strong opinions on both sides of this topic.
Cultural Differences in End-of-Life Decisions
According to Searight and Gafford (2005a), cultural factors strongly influence how doctors, other health care providers, and family members communicate bad news to patients, the expectations regarding who makes the health care decisions, and attitudes about end-of-life care.
In the United States, doctors take the approach that patients should be told the truth about their health. Outside the United States and among certain racial and ethnic groups within the United States, doctors and family members may conceal the full nature of a terminal illness as revealing such information is viewed as potentially harmful to the patient, or at the very least, is seen as disrespectful and impolite. Holland, Geary, Marchini and Tross (1987) found that many doctors in Japan and in numerous African nations used terms such as “mass,” “growth,” and “unclean tissue” rather than referring to cancer when discussing the illness to patients and their families. Family members actively protect terminally ill patients from knowing about their illness in many
Hispanic, Chinese, and Pakistani cultures.[21] In the United States, we view the patient as autonomous in health care decisions[22], while in other nations the family or community plays the main role, or decisions are made primarily by medical professionals, or the doctors in concert with the family make the decisions for the patient. For instance, in comparison to European Americans and African Americans, Koreans and Mexican-Americans are more likely to view family members as the decision makers rather than just the patient[23]. In many Asian cultures, illness is viewed as a “family event,” not just something that impacts the individual patient.[24] Thus, there is an expectation that the family has a say in the health care decisions. As many cultures attribute high regard and respect for doctors, patients and families may defer some of the end-of-life decision making to the medical professionals.[25]
According to a Pew Research Center Survey [26], while death may not be a comfortable topic to ponder, 37% of their survey respondents had given a great deal of thought about their end-of-life wishes, with 35% having put these in writing. Yet, over 25% had given no thought to this issue. Lipka[27]also found that there were clear racial and ethnic differences in end-of-life wishes. Whites are more likely than Blacks and Hispanics to prefer to have treatment stopped if they have a terminal illness. While the majority of Blacks (61%) and Hispanics (55%) prefer that everything be done to keep them alive. Searight and Gafford[28] suggest that the low rate of completion of advance directives among non-whites may reflect a distrust of the U.S. healthcare system as a result of the health care disparities non-whites have experienced. Among Hispanics, patients may also be reluctant to select a single family member to be responsible for end-of-life decisions out of a concern of isolating the person named and of offending other family members, as this is commonly seen as a “family responsibility”[29]
Religious Practices after Death
Funeral rites are expressions of loss that reflect personal and cultural beliefs about the meaning of death and the afterlife. Ceremonies provide survivors a sense of closure after a loss. These rites and ceremonies send the message that the death is real and allow friends and loved ones to express their love and duty to those who die. Under circumstances in which a person has been lost and presumed dead or when family members were unable to attend a funeral, there can continue to be a lack of closure that makes it difficult to grieve and to learn to live with loss. Although many people are still in shock when they attend funerals, the ceremony still provides a marker of the beginning of a new period of one’s life as a survivor. The following are some of the religious practices regarding death, however, individual religious interpretations and practices may occur.[30]
Hindu: The Hindu belief in reincarnation accelerates the funeral ritual, and deceased Hindus are cremated as soon as possible. After being washed, the body is anointed, dressed, and then placed on a stand decorated with flowers ready for cremation. Once the body has been cremated, the ashes are collected and, if possible, dispersed in one of India’s holy rivers.
Judaism: Among the Orthodox, the deceased is first washed and then wrapped in a simple white shroud. Males are also wrapped in their prayer shawls. Once shrouded the body is placed into a plain wooden coffin. The burial must occur as soon as possible after death, and a simple service consisting of prayers and a eulogy is given. After burial the family members typically gather in one home, often that of the deceased, and receive visitors. This is referred to as “sitting shiva.”
Muslim: In Islam the deceased are buried as soon as possible, and it is a requirement that the community be involved in the ritual. The individual is first washed and then wrapped in a plain white shroud called a kaftan. Next, funeral prayers are said followed by the burial. The shrouded dead are placed directly in the earth without a casket and deep enough not to be disturbed. They are also positioned in the earth, on their right side, facing Mecca, Saudi Arabia.
Roman Catholic: Before death an ill Catholic individual is anointed by a priest, commonly referred to as the Anointing of the Sick. The priest recites a prayer and applies consecrated oil to the forehead and hands of the ill person. The individual also takes a final communion consisting of consecrated bread and wine. The funeral rites consist of three parts. First is the wake that usually occurs in a funeral parlor. The body is present and prayers and eulogies are offered by family and friends. The funeral mass is next which includes an opening prayer, bible readings, liturgy, communion, and a concluding rite. The funeral then moves to the cemetery where a blessing of the grave, scripture reading, and prayers conclude the funeral ritual
Bereavement and Grief
The terms grief, bereavement, and mourning are often used interchangeably, however, they have different meanings. Grief is the normal process of reacting to a loss. Grief can be in response to a physical loss, such as a death, or a social loss including a relationship or job. Bereavement is the period after a loss during which grief and mourning occur. Bereavement describes the state of being following the death of someone (bereavement leave). The time spent in bereavement for the loss of a loved one depends on the circumstances of the loss and the level of attachment to the person who died.

Mourning is the process by which people adapt to a loss. Mourning is greatly influenced by cultural beliefs, practices, and rituals.[31]
Four Tasks of Mourning: Worden (2008) identified four tasks that facilitate the mourning process. Worden believes that all four tasks must be completed, but they may be completed in any order and for varying amounts of time. These tasks include:
- Acceptance that the loss has occurred
- Working through the pain of grief
- Adjusting to life without the deceased
- Starting a new life while still maintaining a connection with the deceased
Mourning and funeral rites are expressions of loss that reflect personal and cultural beliefs about the meaning of death and the afterlife. When asked what type of funeral they would like to have, students responded in a variety of ways; each expressing both their personal beliefs and values and those of their culture.
I would like the service to be at a Baptist church, preferably my Uncle Ike’s small church. The service should be a celebration of life . . . I would like there to be hymns sung by my family members, including my favorite one, “It is Well With My Soul”. . .At the end, I would like the message of salvation to be given to the attendees and an altar call for anyone who would like to give their life to Christ. . .
I want a very inexpensive funeral-the bare minimum, only one vase of flowers, no viewing of the remains and no long period of mourning from my remaining family . . . funeral expenses are extremely overpriced and out of hand. . .
When I die, I would want my family members, friends, and other relatives to dress my body as it is usually done in my country, Ghana. Lay my dressed body in an open space in my house at the night prior to the funeral ceremony for my loved ones to walk around my body and mourn for me. . .
I would like to be buried right away after I die because I don’t want my family and friends to see my dead body and to be scared.
In my family we have always had the traditional ceremony-coffin, grave, tombstone, etc. But I have considered cremation and still ponder which method is more favorable. Unlike cremation, when you are ‘buried’ somewhere and family members have to make a special trip to visit, cremation is a little more personal because you can still be in the home with your loved ones . . .
I would like to have some of my favorite songs played....I will have a list made ahead of time. I want a peaceful and joyful ceremony and I want my family and close friends to gather to support one another. At the end of the celebration, I want everyone to go to the Thirsty Whale for a beer and Spang’s for pizza!
When I die, I want to be cremated . . . I want it the way we do it in our culture. I want to have a three day funeral and on the fourth day, it would be my burial/cremation day . . . I want everyone to wear white instead of black, which means they already let go of me. I also want to have a mass on my cremation day.
When I die, I would like to have a befitting burial ceremony as it is done in my Igbo customs. I chose this kind of funeral ceremony because that is what every average person wishes to have.
I want to be cremated . . . I want all attendees wearing their favorite color and I would like the song “Riders on the Storm” to be played . . . I truly hope all the attendees will appreciate the bass. At the end of this simple, short service, attendees will be given multi-colored helium–filled balloons . . . released to signify my release from this earth. . .They will be invited back to the house for ice cream cones, cheese popcorn and a wide variety of other treats and much, much, much rock music . . .
I want to be cremated when I die. To me, it’s not just my culture to do so but it’s more peaceful to put my remains or ashes to the world. Let it free and not stuck in a casket.
Ceremonies provide survivors a sense of closure after a loss. These rites and ceremonies send the message that the death is real and allow friends and loved ones to express their love and duty to those who die. Under circumstances in which a person has been lost and presumed dead or when family members were unable to attend a funeral, there can continue to be a lack of closure that makes it difficult to grieve and to learn to live with loss. And although many people are still in shock when they attend funerals, the ceremony still provides a marker of the beginning of a new period of one’s life as a survivor.
Grief
Grief is the psychological, physical, and emotional experience of loss. The five stages of loss are experienced by those who are in grief (Kubler-Ross & Kessler, 2005). Grief reactions vary depending on whether a loss was anticipated or unexpected, (parents do not expect to lose their children, for example), and whether or not it occurred suddenly or after a long illness, and whether or not the survivor feels responsible for the death.
Struggling with the question of responsibility is particularly felt by those who lose a loved one to suicide. There are numerous survivors for every suicide resulting in 4.5 million survivors of suicide in the United States (American Association of Suicidology, 2007). These survivors may torment themselves with endless “what ifs” in order to make sense of the loss and reduce feelings of guilt. And family members may also hold one another responsible for the loss. The same may be true for any sudden or unexpected death making conflict an added dimension to grief. Much of this laying of responsibility is an effort to think that we have some control over these losses; the assumption being that if we do not repeat the same mistakes, we can control what happens in our life.
Anticipatory grief occurs when a death is expected and survivors have time to prepare to some extent before the loss. Anticipatory grief can include the same denial, anger, bargaining, depression, and acceptance experienced in loss. This can make adjustment after a loss somewhat easier, although the stages of loss will be experienced again after the death (Kubler-Ross & Kessler, 2005). A death after a long-term, painful illness may bring family members a sense of relief that the suffering is over. The exhausting process of caring for someone who is ill is over.
Disenfranchised grief may be experienced by those who have to hide the circumstances of their loss or whose grief goes unrecognized by others. Loss of an ex-spouse, lover, or pet may be examples of disenfranchised grief.
Yet grief continues as long as there is a loss. It has been said that intense grief lasts about two years or less, but grief is felt throughout life. One loss triggers the feelings that surround another. People grieve with varied intensity throughout the remainder of their lives. It does not end. But it eventually becomes something that a person has learned to live with. As long as we experience loss, we experience grief .[32]
There are layers of grief. Initial denial, marked by shock and disbelief in the weeks following a loss may become an expectation that the loved one will walk in the door. And anger directed toward those who could not save our loved one’s life, may become anger that life did not turn out as we expected. There is no right way to grieve. A bereavement counselor expressed it well by saying that grief touches us on the shoulder from time to time throughout life.
Grief and mixed emotions go hand in hand. A sense of relief is accompanied by regrets and periods of reminiscing about our loved ones are interspersed with feeling haunted by them in death. Our outward expressions of loss are also sometimes contradictory. We want to move on but at the same time are saddened by going through a loved one’s possessions and giving them away. We may no longer feel sexual arousal or we may want sex to feel connected and alive. We need others to befriend us but may get angry at their attempts to console us. These contradictions are normal and we need to allow ourselves and others to grieve in their own time and in their own ways.
The “death-denying, grief-dismissing world” is the modern world.[33] We are asked to grieve privately, quickly, and to medicate our suffering. Employers grant us 3 to 5 days for bereavement, if our loss is that of an immediate family member. And such leaves are sometimes limited to no more than one per year. Yet grief takes much longer and the bereaved are seldom ready to perform well on the job. Obviously, life does have to continue. But Kubler-Ross and Kessler suggest that contemporary American society would do well to acknowledge and make more caring accommodations to those who are in grief.
Dual-Process Model of Grieving: The dual-process model takes into consideration that bereaved individuals move back and forth between grieving and preparing for life without their loved one.[34] This model focuses on a loss orientation, which emphasizes the feelings of loss and yearning for the deceased and a
restoration orientation, which centers on the grieving individual re-establishing roles and activities they had prior to the death of their loved one. When oriented toward loss grieving
individuals look back, and when oriented toward restoration they look forward. As one cannot look both back and forward at the same time, a bereaved person must shift back and forth
between the two. Both orientations facilitate normal grieving and interact until bereavement has completed.
Conclusion
Death and grief are topics that are being given greater consideration. This trend should continue as the population “grays” and our awareness of natural disaster and war, both in the United States and throughout the world grows. Viewing death as an integral part of the lifespan will benefit those who are ill, those who are bereaved, and all of us as friends, caregivers, partners, family members, and humans in a global society.
Chapter 12 Key terms
| Physiological death | Living will |
| Social death | Euthanasia |
| Psychic death | Grief |
| Curative care | Bereavement |
| Palliative care | Mourning |
| Hospice | Dual-Process Model of Grieving |
| advance directive |
Attribution
This chapter is from Development through the Lifespan by Maricopa College. The Maricopa chapter on Death and Dying is adapted from Module 11 Death and Dying in Lifespan Development by Lumen Learning licensed under a CC BY license. The Lumen work uses content from Psyc 200 Lifespan Psychology by Laura Overstreet shared with a CC BY license.
- Overstreet, Laura. Personal Notes. Psyc 200 Lifespan Psychology. ↵
- (Pattison, 1977) ↵
- CDC ↵
- Batts, 2004; Erber & Szuchman, 2015; National Cancer Institute, 2013). ↵
- (1969, 1975) ↵
- (Maciejewski, Zhang, Block, & Prigerson, 2007) ↵
- (Fox, 1997) ↵
- (NHPCO, 2014). ↵
- (National Center for Health Statistics, 2003). ↵
- (Weitz, 2007). ↵
- (APA Online, 2001). ↵
- (Wolfe et al., in Berger, 2005). ↵
- (Hospital Foundation of America, 2009). ↵
- Institute of Medicine(2015) ↵
- (IOM, 2015) ↵
- Redfoot, Feinberg, & Houser, 2013 ↵
- Adapted from IOM, 2015 ↵
- (IOM, 2015) ↵
- (IOM, 2015, p. 18). ↵
- (Oregon Public Health Division, 2016) ↵
- (Kaufert & Putsch, 1997; Herndon & Joyce, 2004 ↵
- (Searight & Gafford, 2005a) ↵
- (Berger, 1998; Searight & Gafford, 2005a) ↵
- (Candib, 2002) ↵
- (Searight & Gafford, 2005b ↵
- (Lipka, 2014) ↵
- (2014) ↵
- (2005a) ↵
- Morrison, Zayas, Mulvihill, Baskin, & Meier, 1998 ↵
- (Dresser & Wasserman, 2010; Schechter, 2009). ↵
- (Casarett, Kutner, & Abrahm, 2001 ↵
- (Kubler-Ross & Kessler, 2005). ↵
- (Kubler-Ross & Kessler, 2005, p. 205). ↵
- (Stroebe & Schut, 2001; Stroebe, Schut, & Stroebe, 2005 ↵
