
Interaction of Model of Communication
The Interaction Model of communication (see Figure 1.4) describes communication as a process in which participants alternate positions as sender and receiver and generate meaning by sending messages and receiving feedback within physical and psychological contexts (Schramm, 1997). Rather than illustrating communication as a linear, one-way process, this model incorporates feedback, which makes communication a more interactive, two-way process.
Feedback includes messages sent in response to other messages. For example, a patient may ask you a question in response to health information you provide them. The inclusion of a feedback loop allows a more complex understanding of the roles of participants in a communication encounter. Rather than having one sender, one message, and one receiver, this model has two sender-receivers who exchange messages. Each participant alternates roles as sender and receiver in order to keep a communication encounter going. You alternate between the roles of sender and receiver very quickly and often without conscious thought.
The Interaction Model of communication is more interaction-focused. In this model, communication isn’t judged as effective or ineffective based on whether or not a single message was successfully transmitted and received. In fact, this model acknowledges that because so many messages may be sent at one time, many of them may not even be received. Some messages are also unintentionally sent. Thus, the model acknowledges that communication is nuanced and complex.
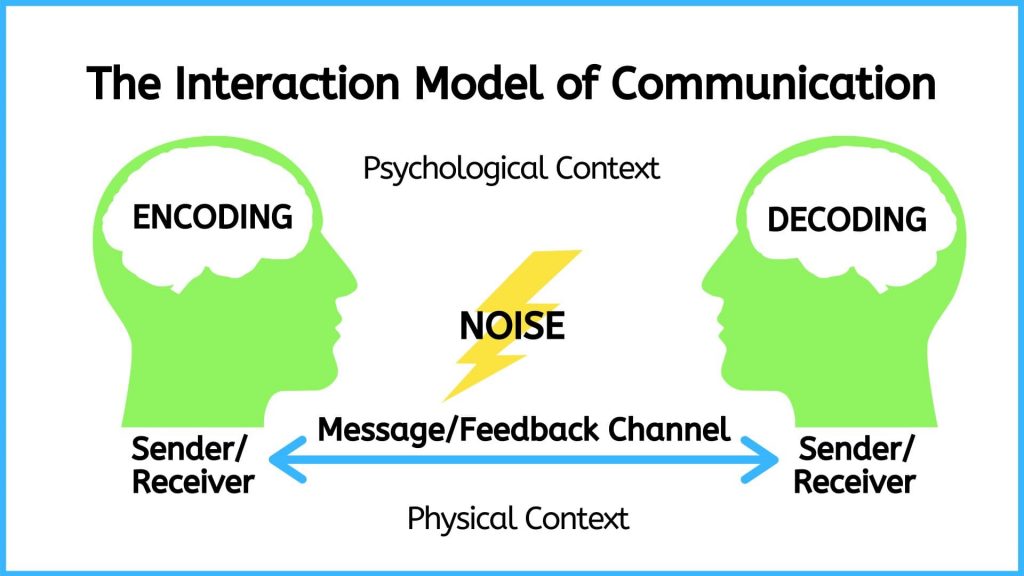
Figure 1.4: The Interaction Model of Communication
The Interaction Model takes physical and psychological context into account.
- Physical context includes the environmental factors in a communication encounter. The size, layout, temperature, and lighting of a space influence your communication. Imagine the different physical contexts in which the nurse-client encounter takes place and how this can affect communication. You may be attempting to have an emotionally laden discussion with a client in a room where the beds are only separated by curtains. You may be assessing a client in the community where the lighting is dim. Whether it’s the size of the room, the temperature, or other environmental factors, it’s important to consider the role that physical context plays in communication.
- Psychological context includes the mental and emotional factors in a communication encounter. Stress, anxiety, and emotions are just some examples of psychological influences that can affect communication. For example, you may be communicating with a client who is in pain and afraid in the emergency room. You may be introducing yourself to one client, but worried about another client who is grieving. Alternatively, you may be communicating with groups of clients and families who are experiencing myriad of emotions.
Nursing Example
A nurse has worked 11 hours and is attending to a client recently admitted to the hospital. The 68-year-old client is waiting for a bed and is stationed on a stretcher in the emergency room hallway. The client sought emergency care after experiencing severe abdominal pain and passing substantial blood when having a bowel movement. The client was informed that it is likely they have end-stage bowel cancer but is still awaiting a formal diagnosis and referral to oncology (cancer specialist). The nurse asks the client if the nurse can take a set of vital signs. The client responds “yes.” The nurse also tries to make the client comfortable by adjusting the head of the stretcher and asks the client if they need anything. The client has many questions and concerns and has not had anything to eat or drink in several hours but responds “no.” The nurse says “OK, well let me know if you need anything.”
Analysis: The physical context that played an important role in this example is the lack of privacy and overstimulation in a waiting area located in an emergency room hallway. The physical space likely played a role in the client’s response, which resulted in the client’s needs being unmet. The psychological context relates to the burden of a looming terminal diagnosis juxtaposed with the undignified environment. The nurse may have sensed that probing further about the client’s needs and current state of mind was needed but may have been physically tired and emotionally drained after working 11 hours. All these factors contributed to the interaction between the nurse and the client.
Pros: This model allows the user to reflect on the environment (both physical and psychological) and how this contributes to good communication. In this case, communication was deemed inadequate because the interaction was limited by the environmental context.
Cons: Although this model attends to the broader context in which communication takes place, it is also inattentive to social, political, and economic realities that shape communication. In other words, it does not consider how the nurse’s and the client’s identity inform their communication with each other.
Attribution Statement
Remixed with original content and adapted, with editorial changes, from:
Communication in the Real World: An Introduction to Communication Studies by University of Minnesota. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.
