
11.4 Two Fundamental Human Motivations: Eating and Mating
Learning Objectives
- Understand the biological and social responses that underlie eating behaviour.
- Understand the psychological and physiological responses that underlie sexual behaviour.
Eating: Healthy Choices Make Healthy Lives
Along with the need to drink fresh water, which humans can normally attain in all except the most extreme situations, the need for food is the most fundamental and important human need. More than one in 10 Canadian households contain people who live without enough nourishing food, and this lack of proper nourishment has profound effects on their abilities to lead productive lives (Yarema, 2013). When people are extremely hungry, their motivation to attain food completely changes their behaviour. Hungry people become listless and apathetic to save energy and then become completely obsessed with food. Ancel Keys and his colleagues (Keys, Brožek, Henschel, Mickelsen, & Taylor, 1950) found that volunteers who were placed on severely reduced-calorie diets lost all interest in sex and social activities, becoming preoccupied with food.
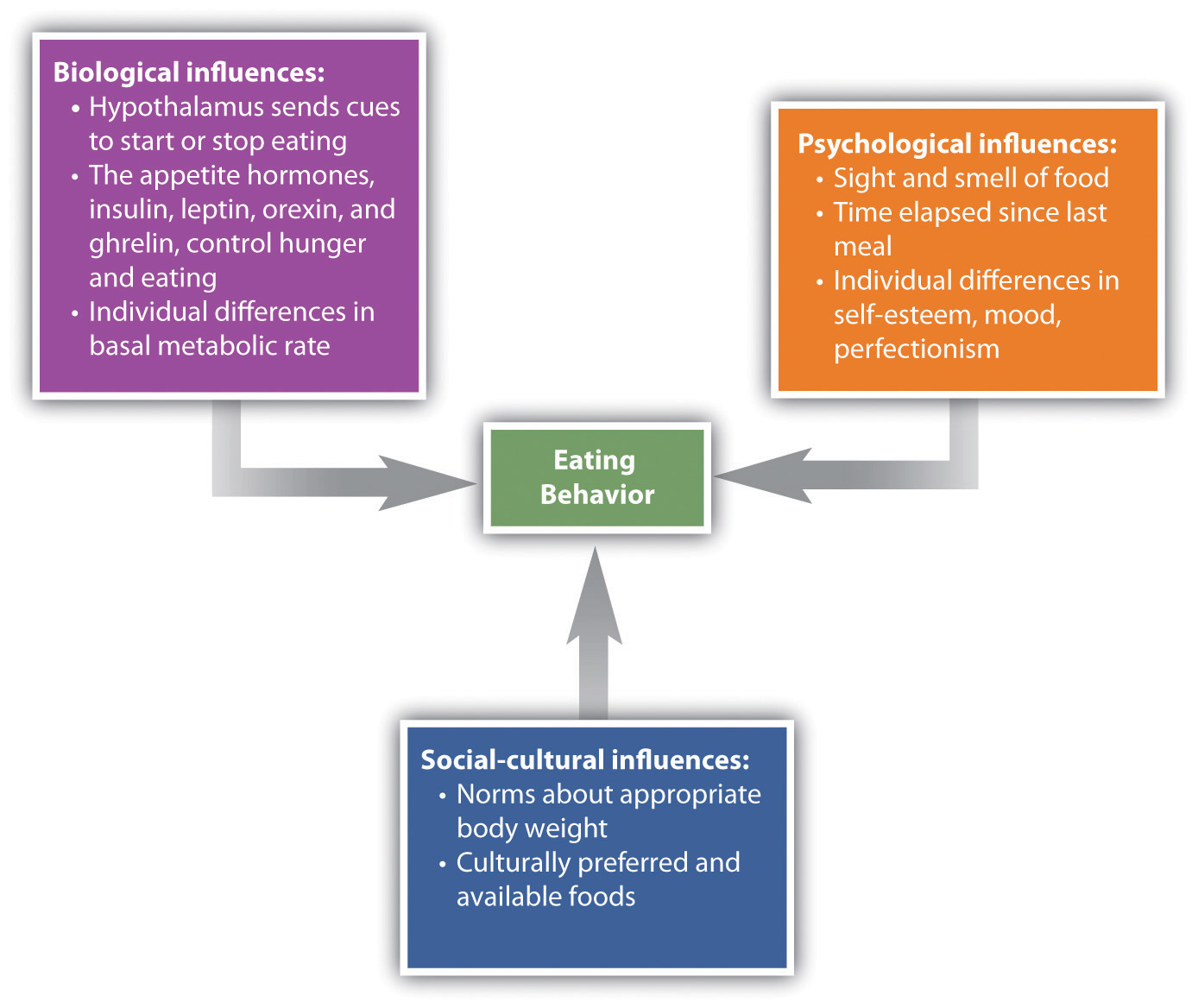
Like most interesting psychological phenomena, the simple behaviour of eating has both biological and social determinants (Figure 11.11, “Biological, Psychological, and Social-Cultural Contributors to Eating”). Biologically, hunger is controlled by the interactions among complex pathways in the nervous system and a variety of hormonal and chemical systems in the brain and body. The stomach is of course important. We feel more hungry when our stomach is empty than when it is full. But we can also feel hunger even without input from the stomach. Two areas of the hypothalamus are known to be particularly important in eating. The lateral part of the hypothalamus responds primarily to cues to start eating, whereas the ventromedial part of the hypothalamus primarily responds to cues to stop eating. If the lateral part of the hypothalamus is damaged, the animal will not eat even if food is present, whereas if the ventromedial part of the hypothalamus is damaged, the animal will eat until it is obese (Wolf & Miller, 1964).
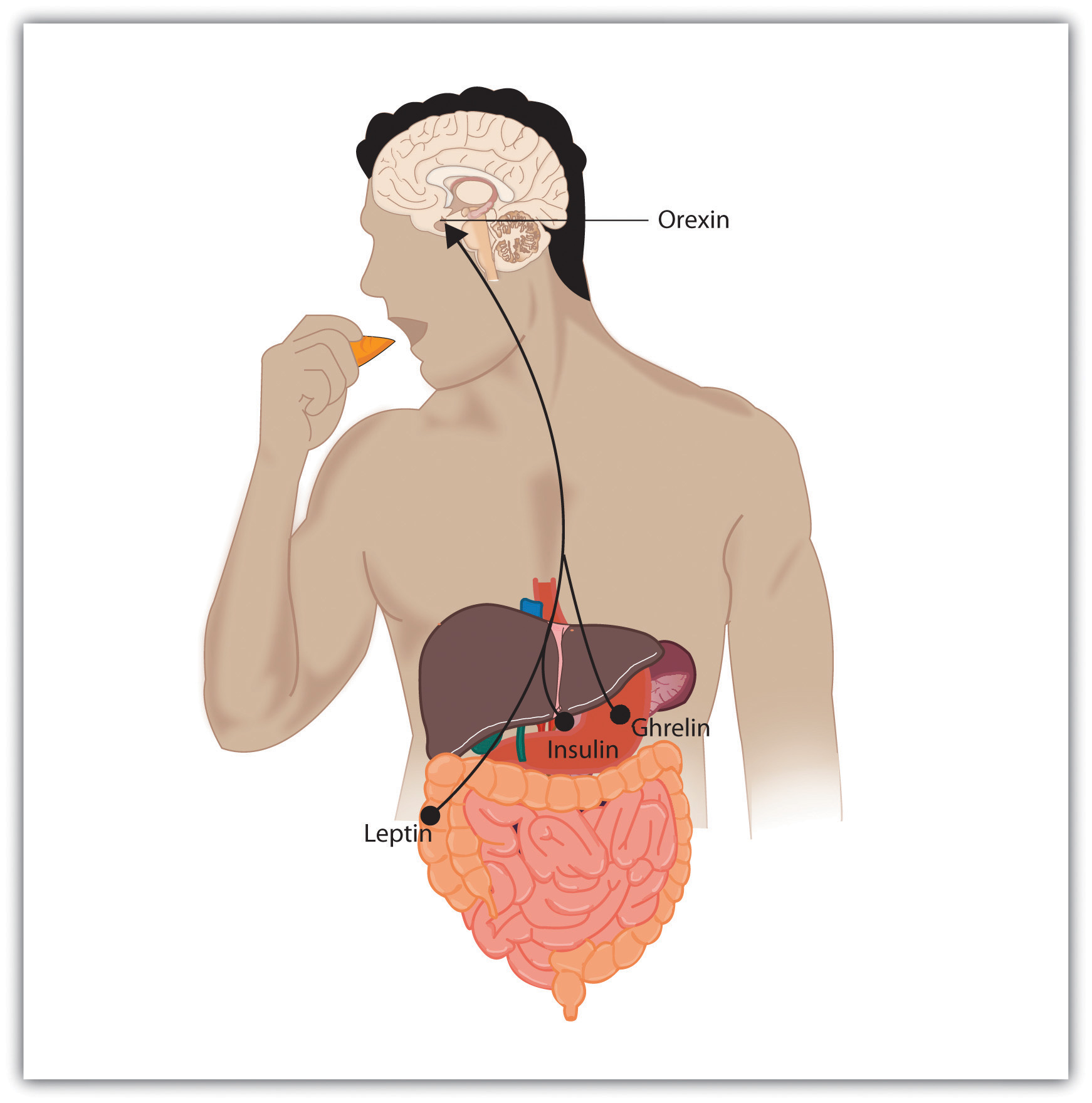
Hunger is also determined by hormone levels (Figure 11.12, “Eating Is Influenced by the Appetite Hormones”). Glucose is the main sugar that the body uses for energy, and the brain monitors blood glucose levels to determine hunger. Glucose levels in the bloodstream are regulated by insulin, a hormone secreted by the pancreas gland. When insulin is low, glucose is not taken up by body cells, and the body begins to use fat as an energy source. Eating and appetite are also influenced by other hormones, including orexin, ghrelin, and leptin (Brennan & Mantzoros, 2006; Nakazato et al., 2001).
Normally the interaction of the various systems that determine hunger creates a balance or homeostasis in which we eat when we are hungry and stop eating when we feel full. But homeostasis varies among people; some people simply weigh more than others, and there is little they can do to change their fundamental weight. Weight is determined in large part by the basal metabolic rate, the amount of energy expended while at rest. Each person’s basal metabolic rate is different, due to his or her unique physical makeup and physical behaviour. A naturally occurring low metabolic rate, which is determined entirely by genetics, makes weight management a very difficult undertaking for many people.
How we eat is also influenced by our environment. When researchers rigged clocks to move faster, people got hungrier and ate more, as if they thought they must be hungry again because so much time had passed since they last ate (Schachter, 1968). And if we forget that we have already eaten, we are likely to eat again even if we are not actually hungry (Rozin, Dow, Moscovitch, & Rajaram, 1998).
Cultural norms about appropriate weights also influence eating behaviours. Current norms for women in Western societies are based on a very thin body ideal, emphasized by television and movie actresses, models, and even children’s dolls, such as the ever-popular Barbie. These norms for excessive thinness are very difficult for most women to attain: Barbie’s measurements, if translated to human proportions, would be about 91 cm-46 cm-84 cm at bust-waist-hips, measurements that are attained by less than one in 100,000 women (Norton, Olds, Olive, & Dank, 1996). Many women idealize being thin and yet are unable to reach the standard that they prefer.
Eating Disorders
In some cases, the desire to be thin can lead to eating disorders, which are estimated to affect about 1% of people, 90% of them women (Hoek & van Hoeken, 2003; Palmer, 2008; Patrick, 2002). Anorexia nervosa is an eating disorder characterized by extremely low body weight, distorted body image, and an obsessive fear of gaining weight. Anorexia begins with a severe weight loss diet and develops into a preoccupation with food and dieting.
Bulimia nervosa is an eating disorder characterized by binge eating followed by purging. Bulimia nervosa begins after the dieter has broken a diet and gorged. Bulimia involves repeated episodes of overeating, followed by vomiting, laxative use, fasting, or excessive exercise. It is most common in women in their late teens or early 20s, and it is often accompanied by depression and anxiety, particularly around the time of the binging. The cycle in which the person eats to feel better, but then after eating becomes concerned about weight gain and purges, repeats itself over and over again, often with major psychological and physical results.
Eating disorders are in part heritable (Klump, Burt, McGue, & Iacono, 2007), and it is not impossible that at least some have been selected through their evolutionary significance in coping with food shortages (Guisinger, 2008). Eating disorders are also related to psychological causes, including low self-esteem, perfectionism, and the perception that one’s body weight is too high (Vohs et al., 2001), as well as to cultural norms about body weight and eating (Crandall, 1988). Because eating disorders can create profound negative health outcomes, including death, people who suffer from them should seek treatment. This treatment is often quite effective.
Obesity
Although some people eat too little, eating too much is also a major problem. Obesity is a medical condition in which so much excess body fat has accumulated in the body that it begins to have an adverse impact on health. In addition to causing people to be stereotyped and treated less positively by others (Crandall, Merman, & Hebl, 2009), uncontrolled obesity leads to health problems including cardiovascular disease, diabetes, sleep apnea, arthritis, Alzheimer’s disease, and some types of cancer (Gustafson, Rothenberg, Blennow, Steen, & Skoog, 2003). Obesity also reduces life expectancy (Haslam & James, 2005).
Obesity is determined by calculating the body mass index (BMI), a measurement that compares one’s weight and height. People are defined as overweight when their BMI is greater than 25 kg/m2 and as obese when it is greater than 30 kg/m2. If you know your height and weight, you can calculate your BMI (https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm)
Obesity is a leading cause of death worldwide. Its prevalence is rapidly increasing, and it is one of the most serious public health problems of the 21st century. Although obesity is caused in part by genetics, it is increased by overeating and a lack of physical activity (James, 2008; Nestle & Jacobson, 2000).
There are really only two approaches to controlling weight: eat less and exercise more. Dieting is difficult for anyone, but it is particularly difficult for people with slow basal metabolic rates who must cope with severe hunger to lose weight. Although most weight loss can be maintained for about a year, very few people are able to maintain substantial weight loss through dieting alone for more than three years (Miller, 1999). Substantial weight loss of more than 50 pounds is typically seen only when weight loss surgery has been performed (Douketis, Macie, Thabane, & Williamson, 2005). Weight loss surgery reduces stomach volume or bowel length, leading to earlier satiation and reduced ability to absorb nutrients from food.
Although dieting alone does not produce a great deal of weight loss over time, its effects are substantially improved when it is accompanied by more physical activity. People who exercise regularly, and particularly those who combine exercise with dieting, are less likely to be obese (Borer, 2008). Exercise not only improves our waistline but also makes us healthier overall. Exercise increases cardiovascular capacity, lowers blood pressure, and helps improve diabetes, joint flexibility, and muscle strength (American Heart Association, 1998). Exercise also slows the cognitive impairments that are associated with aging (Kramer, Erickson, & Colcombe, 2006).
Because the costs of exercise are immediate but the benefits are long-term, it may be difficult for people who do not exercise to get started. It is important to make a regular schedule, to work exercise into one’s daily activities, and to view exercise not as a cost but as an opportunity to improve oneself (Schomer & Drake, 2001). Exercising is more fun when it is done in groups, so team exercise is recommended (Kirchhoff, Elliott, Schlichting, & Chin, 2008).
A recent report found that only about one-half of North Americans perform the 30 minutes of exercise five times a week that the World Health Organization (2010) suggests as the minimum healthy amount. As for the other half of North Americans, they most likely are listening to the guidelines, but they are unable to stick to the regimen. Almost half of the people who start an exercise regimen give it up by the six-month mark (American Heart Association, 1998; Colley, Garriguet, Janssen, Craig, Clarke, & Tremblay, 2011).
Statistics Canada (2010) also reports just 7% of young people between the ages of five and 17 meet the daily recommended amount of physical activity. New international and proposed Canadian guidelines recommend adults accumulate at least 150 minutes of moderate-to-vigorous physical activity a week to obtain substantial health benefits. The guidelines also suggest five- to 17-year-olds should accumulate at least 60 minutes of moderate-to-vigorous physical activity daily. Statistics Canada says the guidelines for adults were achieved by 17% of men and 14% of women, while the youth guidelines were met by just 9% of boys and 4% of girls. This is a problem, given that exercise has long-term benefits only if it is continued.
Sex: The Most Important Human Behaviour
Perhaps the most important aspect of human experience is the process of reproduction. Without it, none of us would be here. Successful reproduction in humans involves the coordination of a wide variety of behaviours, including courtship, sex, household arrangements, parenting, and child care.
The Experience of Sex
The sexual drive, with its reward of intense pleasure in orgasm, is highly motivating. The biology of the sexual response was studied in detail by Masters and Johnson (1966), who monitored or filmed more than 700 men and women while they masturbated or had intercourse. Masters and Johnson found that the sexual response cycle—the biological sexual response in humans—was very similar in men and women, and consisted of four stages:
- Excitement. The genital areas become engorged with blood. Women’s breasts and nipples may enlarge and the vagina expands and secretes lubricant.
- Plateau. Breathing, pulse, and blood pressure increase as orgasm feels imminent. The penis becomes fully enlarged. Vaginal secretions continue and the clitoris may retract.
- Orgasm. Muscular contractions occur throughout the body, but particularly in the genitals. The spasmodic ejaculations of sperm are similar to the spasmodic contractions of vaginal walls, and the experience of orgasm is similar for men and women. The woman’s orgasm helps position the uterus to draw sperm inward (Thornhill & Gangestad, 1995).
- Resolution. After orgasm the body gradually returns to its prearoused state. After one orgasm, men typically experience a refractory period, in which they are incapable of reaching another orgasm for several minutes, hours, or even longer. Women may achieve several orgasms before entering the resolution stage.
The sexual response cycle and sexual desire are regulated by the sex hormones estrogen in women and testosterone in both women and in men. Although the hormones are secreted by the ovaries and testes, it is the hypothalamus and the pituitary glands that control the process. Estrogen levels in women vary across the menstrual cycle, peaking during ovulation (Pillsworth, Haselton, & Buss, 2004). Women are more interested in having sex during ovulation but can experience high levels of sexual arousal throughout the menstrual cycle.
In men, testosterone is essential to maintain sexual desire and to sustain an erection, and testosterone injections can increase sexual interest and performance (Aversa et al., 2000; Jockenhövel et al., 2009). Testosterone is also important in the female sex cycle. Women who are experiencing menopause may develop a loss of interest in sex, but this interest may be rekindled through estrogen and testosterone replacement treatments (Meston & Frohlich, 2000).
Although their biological determinants and experiences of sex are similar, men and women differ substantially in their overall interest in sex, the frequency of their sexual activities, and the mates they are most interested in. Men show a more consistent interest in sex, whereas the sexual desires of women are more likely to vary over time (Baumeister, 2000). Men fantasize about sex more often than women, and their fantasies are more physical and less intimate (Leitenberg & Henning, 1995). Men are also more willing to have casual sex than are women, and their standards for sex partners is lower (Petersen & Hyde, 2010; Saad, Eba, & Sejean, 2009).
Gender differences in sexual interest probably occur in part as a result of the evolutionary predispositions of men and women, and this interpretation is bolstered by the finding that gender differences in sexual interest are observed cross-culturally (Buss, 1989). Evolutionarily, women should be more selective than men in their choices of sex partners because they must invest more time in bearing and nurturing their children than men do (most men do help out, of course, but women simply do more [Buss & Kenrick, 1998]). Because they do not need to invest a lot of time in child rearing, men may be evolutionarily predisposed to be more willing and desiring of having sex with many different partners and may be less selective in their choice of mates. Women, on the other hand, because they must invest substantial effort in raising each child, should be more selective.
The Many Varieties of Sexual Behaviour
Sex researchers have found that sexual behaviour varies widely, not only between men and women but within each sex (Kinsey, Pomeroy, & Martin, 1948/1998; Kinsey, 1953/1998). About a quarter of women report having a low sexual desire, and about 1% of people report feeling no sexual attraction whatsoever (Bogaert, 2004; Feldhaus-Dahir, 2009; West et al., 2008). There are also people who experience hyperactive sexual drives. For about 3% to 6% of the population (mainly men), the sex drive is so strong that it dominates life experience and may lead to hyperactive sexual desire disorder (Kingston & Firestone, 2008).
There is also variety in sexual orientation, which is the direction of our sexual desire toward people of the opposite sex, people of the same sex, or people of both sexes. The vast majority of human beings have a heterosexual orientation — their sexual desire is focused toward members of the opposite sex. A smaller minority is primarily homosexual (i.e., they have sexual desire for members of their own sex). Between 3% and 4% of men are gay, and between 1% and 2% of women are lesbian. Another 1% of the population reports being bisexual (having desires for both sexes). The love and sexual lives of homosexuals are little different from those of heterosexuals, except where their behaviours are constrained by cultural norms and local laws. As with heterosexuals, some gays and lesbians are celibate, some are promiscuous, but most are in committed, long-term relationships (Laumann, Gagnon, Michael, & Michaels, 1994).
Although homosexuality has been practiced as long as records of human behaviour have been kept, and occurs in many animals at least as frequently as it does in humans, cultures nevertheless vary substantially in their attitudes toward it. In Western societies such as the Canada, the United States, and Europe, attitudes are becoming progressively more tolerant of homosexuality, but it remains unacceptable in many other parts of the world. The Canadian Psychological Association issued a policy statement in February 1982 endorsing the principle that there be no discrimination on the basis of sexual orientation for (a) recruitment; (b) hiring; (c) salary; (d) promotion rate; (e) fringe benefits; or (f) assignment of duties. The American Psychiatric Association no longer considers homosexuality to be a mental illness, although it did so until 1973. Because prejudice against gays and lesbians can lead to experiences of ostracism, depression, and even suicide (Kulkin, Chauvin, & Percle, 2000), these improved attitudes can benefit the everyday lives of gays, lesbians, and bisexuals.
Whether sexual orientation is driven more by nature or by nurture has received a great deal of research attention, and research has found that sexual orientation is primarily biological (Mustanski, Chivers, & Bailey, 2002). Areas of the hypothalamus are different in homosexual men, as well as in animals with homosexual tendencies, than they are in heterosexual members of the species, and these differences are in directions such that gay men are more similar to women than straight men are (Gladue, 1994; Lasco, Jordan, Edgar, Petito, & Byrne, 2002; Rahman & Wilson, 2003). Twin studies also support the idea that there is a genetic component to sexual orientation. Among male identical twins, 52% of those with a gay brother also reported homosexuality, whereas the rate in fraternal twins was just 22% (Bailey et al., 1999; Pillard & Bailey, 1998). There is also evidence that sexual orientation is influenced by exposure and responses to sex hormones (Hershberger & Segal, 2004; Williams & Pepitone, 2000).
Psychology in Everyday Life: Regulating Emotions to Improve Our Health
Although smoking cigarettes, drinking alcohol, using recreational drugs, engaging in unsafe sex, and eating too much may produce enjoyable positive emotions in the short term, they are some of the leading causes of negative health outcomes and even death in the long term (Mokdad, Marks, Stroup, & Gerberding, 2004). To avoid these negative outcomes, we must use our cognitive resources to plan, guide, and restrain our behaviours. And we (like Gavin England) can also use our emotion regulation skills to help us do better.
Even in an age where the addictive and detrimental health effects of cigarette smoking are well understood, more than 60% of children try smoking before they are 18 years old, and more than half who have smoked have tried and failed to quit (Fryar, Merino, Hirsch, & Porter, 2009). Although smoking is depicted in movies as sexy and alluring, it is highly addictive and probably the most dangerous thing we can do to our body. Poor diet and physical inactivity combine to make up the second greatest threat to our health. But we can improve our diet by eating more natural and less processed food, and by monitoring our food intake. And we can start and maintain an exercise program. Exercise keeps us happier, improves fitness, and leads to better health and lower mortality (Fogelholm, 2010; Galper, Trivedi, Barlow, Dunn, & Kampert, 2006; Hassmén, Koivula, & Uutela, 2000). And exercise also has a variety of positive influences on our cognitive processes, including academic performance (Hillman, Erickson, & Kramer, 2008).
Alcohol abuse, and particularly binge drinking (i.e., having five or more drinks in one sitting), is often the norm among high school and university students, but it has severe negative health consequences. Bingeing leads to deaths from car crashes, drowning, falls, gunshots, and alcohol poisoning (Valencia-Martín, Galán, & Rodríguez-Artalejo, 2008). Binge-drinking students are also more likely to be involved in other risky behaviours, such as smoking, drug use, dating violence, or attempted suicide (Miller, Naimi, Brewer, & Jones, 2007). Binge drinking may also damage neural pathways in the brain (McQueeny et al., 2009) and lead to lifelong alcohol abuse and dependency (Kim et al., 2008). Illicit drug use has also been increasing and is linked to the spread of infectious diseases such as HIV, hepatitis B, and hepatitis C (Monteiro, 2001).
Some teens abstain from sex entirely, particularly those who are very religious, but most experiment with it. In Canada, 30% of 15- to 17-year-olds and 68% of 18- to 19-year-olds reported that they had had intercourse (Rotermann, 2012). In sum, while less than half of Canadian teens report having intercourse before age 18, more than two-thirds do so before age 20. When these data are added to data from previous cycles of the Canadian Community Health Survey we can see that the percentages of Canadian young people in the 15- to 17- and 18- to 19-year-old age groups who reported ever having sexual intercourse remained remarkably stable from 1996/1997 to 2009/2010. Although sex is fun, it can also kill us if we are not careful. Sexual activity can lead to guilt about having engaged in the act itself, and may also lead to unwanted pregnancies and sexually transmitted infections (STIs), including HIV infection. Alcohol consumption also leads to risky sexual behaviour. Sex partners who have been drinking are less likely to practice safe sex, and they have an increased risk of STIs, including HIV infection (Hutton, McCaul, Santora, & Erbelding 2008; Raj et al., 2009).
It takes some work to improve and maintain our health and happiness, and our desire for the positive emotional experiences that come from engaging in dangerous behaviours can get in the way of this work. But being aware of the dangers, working to control our emotions, and using our resources to engage in healthy behaviours and avoid unhealthy ones are the best things we can do for ourselves.
Key Takeaways
- Biologically, hunger is controlled by the interactions among complex pathways in the nervous system and a variety of hormonal and chemical systems in the brain and body.
- How we eat is also influenced by our environment, including social norms about appropriate body size.
- Homeostasis varies among people and is determined by the basal metabolic rate. Low metabolic rates, which are determined entirely by genetics, make weight management a very difficult undertaking for many people.
- Eating disorders, including anorexia nervosa and bulimia nervosa, affect about 1% of people (90% women).
- Obesity is a medical condition in which so much excess body fat has accumulated in the body that it begins to have an adverse impact on health. Uncontrolled obesity leads to health problems including cardiovascular disease, diabetes, sleep apnea, arthritis, and some types of cancer.
- The two approaches to controlling weight are to eat less and exercise more.
- Sex drive is regulated by the sex hormones estrogen in women and testosterone in both women and men.
- Although their biological determinants and experiences of sex are similar, men and women differ substantially in their overall interest in sex, the frequency of their sexual activities, and the mates they are most interested in.
- Sexual behaviour varies widely, not only between men and women but also within each sex.
- There is also variety in sexual orientation: toward people of the opposite sex, people of the same sex, or people of both sexes. The determinants of sexual orientation are primarily biological.
- We can outwit stress, obesity, and other health risks through appropriate healthy action.
Exercise and Critical Thinking
- Consider your own eating and sex patterns. Are they healthy or unhealthy? What can you do to improve them?
References
American Heart Association. (1998). Statement on exercise, benefits and recommendations for physical activity programs for all Americans. American Heart Association, 94, 857–862. Retrieved from http://circ.ahajournals.org/cgi/content/full/94/4/857?ijkey=6e9ad2e53ba5b25f9002a707e5e4b5b8ee015481&keytype2=tf_ipsecsha.
Aversa, A., Isidori, A., De Martino, M., Caprio, M., Fabbrini, E., Rocchietti-March, M.,…Fabri, A. (2000). Androgens and penile erection: evidence for a direct relationship between free testosterone and cavernous vasodilation in men with erectile dysfunction. Clinical Endocrinology, 53(4), 517–522.
Bailey, J., Pillard, R., Dawood, K., Miller, M., Farrer, L., Shruti Trivedi, L.,…Murphy, R. L. (1999). A family history study of male sexual orientation using three independent samples. Behavior Genetics, 29(2), 79–86. Retrieved from Academic Search Premier Database.
Baumeister, R. F. (2000). Gender differences in erotic plasticity: The female sex drive as socially flexible and responsive. Psychological Bulletin, 126(3), 347–374.
Bogaert, A. (2004). Asexuality: Prevalence and associated factors in a national probability sample. Journal of Sex Research, 41(3), 279–287. Retrieved from Academic Search Premier Database.
Borer, K. T. (2008). How effective is exercise in producing fat loss? Kinesiology, 40(2), 126–137.
Brennan, A. M., & Mantzoros, C. S. (2006). Drug insight: The role of leptin in human physiology and pathophysiology-emerging clinical applications. Nature Clinical Practice Endocrinology Metabolism, 2(6), 318–27.
Buss, D. M. (1989). Sex differences in human mate preferences: Evolutionary hypotheses tested in 37 cultures. Behavioral and Brain Sciences, 12(1), 1–49.
Buss, D., & Kenrick, D. (1998). Evolutionary social psychology. In D. T. Gilbert, S. T. Fiske, & G. Lindzey (Eds.), Handbook of Social Psychology (4th ed., Vol. 2, pp. 982–1026). Boston, MA: McGraw-Hill.
Colley, R. C., Garriguet, D., Janssen, I., Craig, C. L., Clarke, J., & Tremblay, M. S. (2011). Physical activity of Canadian adults: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Statistics Canada.
Crandall, C. S. (1988). Social contagion of binge eating. Journal of Personality & Social Psychology, 55(4), 588–598.
Crandall, C. S., Merman, A., & Hebl, M. (2009). Anti-fat prejudice. In T. D. Nelson (Ed.), Handbook of prejudice, stereotyping, and discrimination (pp. 469–487). New York, NY: Psychology Press.
Douketis, J. D., Macie C., Thabane, L., & Williamson, D. F. (2005). Systematic review of long-term weight loss studies in obese adults: Clinical significance and applicability to clinical practice. International Journal of Obesity, 29, 1153–1167.
Feldhaus-Dahir, M. (2009). The causes and prevalence of hypoactive sexual desire disorder: Part I. Urologic Nursing, 29(4), 259–263. Retrieved from Academic Search Premier Database.
Fogelholm, M. (2010). Physical activity, fitness and fatness: Relations to mortality, morbidity and disease risk factors. A systematic review. Obesity Reviews, 11(3), 202–221.
Fryar, C. D., Merino, M. C., Hirsch, R., & Porter, K. S. (2009). Smoking, alcohol use, and illicit drug use reported by adolescents aged 12–17 years: United States, 1999–2004. National Health Statistics Reports, 15, 1–23.
Galper, D., Trivedi, M., Barlow, C., Dunn, A., & Kampert, J. (2006). Inverse association between physical inactivity and mental health in men and women. Medicine & Science in Sports & Exercise, 38(1), 173–178.
Gladue, B. A. (1994). The biopsychology of sexual orientation. Current Directions in Psychological Science, 3(5), 150–154.
Guisinger, S. (2008). Competing paradigms for anorexia nervosa. American Psychologist, 63(3), 199–200.
Gustafson, D., Rothenberg, E., Blennow, K., Steen, B., & Skoog, I. (2003). An 18-year follow-up of overweight and risk of Alzheimer disease. Archives of Internal Medicine, 163(13), 1524.
Haslam, D. W., & James, W. P. (2005). Obesity. Lancet, 366(9492), 197–209.
Hassmén, P., Koivula, N., & Uutela, A. (2000). Physical exercise and psychological well-being: A population study in Finland. Preventive Medicine: An International Journal Devoted to Practice and Theory, 30(1), 17–25.
Hershberger, S., & Segal, N. (2004). The cognitive, behavioral, and personality profiles of a male monozygotic triplet set discordant for sexual orientation. Archives of Sexual Behavior, 33(5), 497–514. Retrieved from Academic Search Premier Database.
Hillman, C. H., Erickson, K. I., & Kramer, A. F. (2008). Be smart, exercise your heart: Exercise effects on brain and cognition. Nature Reviews Neuroscience, 9(1), 58–65.
Hoek, H. W., & van Hoeken, D. (2003). Review of the prevalence and incidence of eating disorders. International Journal of Eating Disorders, 34(4), 383–396.
Hutton, H., McCaul, M., Santora, P., & Erbelding, E. (2008). The relationship between recent alcohol use and sexual behaviors: Gender differences among sexually transmitted disease clinic patients. Alcoholism: Clinical & Experimental Research, 32(11), 2008–2015.
James, W. P. (2008). The fundamental drivers of the obesity epidemic. Obesity Review, 9(Suppl. 1), 6–13.
Jockenhövel, F., Minnemann, T., Schubert, M., Freude, S., Hübler, D., Schumann, C.,…Ernst, M. (2009). Timetable of effects of testosterone administration to hypogonadal men on variables of sex and mood. Aging Male, 12(4), 113–118.
Keys, A., Brožek, J., Henschel, A., Mickelsen, O., & Taylor, H. L. (1950). The biology of human starvation (Vols. 1–2). Oxford, England: University of Minnesota Press.
Kim, J., Sing, L., Chow, J., Lau, J., Tsang, A., Choi, J.,…Griffiths, S. M. (2008). Prevalence and the factors associated with binge drinking, alcohol abuse, and alcohol dependence: A population-based study of Chinese adults in Hong Kong. Alcohol & Alcoholism, 43(3), 360–370.
Kingston, D. A., & Firestone, P. (2008). Problematic hypersexuality: A review of conceptualization and diagnosis. Sexual Addictions and Compulsivity, 15, 284–310.
Kinsey, A. C. (1998). Sexual behavior in the human female. Bloomington: Indiana University Press. (Original work published 1953)
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1998). Sexual behavior in the human male. Bloomington: Indiana University Press. (Original work published 1948).
Kirchhoff, A., Elliott, L., Schlichting, J., & Chin, M. (2008). Strategies for physical activity maintenance in African American women. American Journal of Health Behavior, 32(5), 517–524. Retrieved from Academic Search Premier Database.
Klump, K. L., Burt, S. A., McGue, M., & Iacono, W. G. (2007). Changes in genetic and environmental influences on disordered eating across adolescence: A longitudinal twin study. Archives of General Psychiatry, 64(12), 1409–1415.
Kramer, A. F., Erickson, K. I., & Colcombe, S. J. (2006). Exercise, cognition, and the aging brain. Journal of Applied Physiology, 101(4), 1237–1242.
Kulkin, H. S., Chauvin, E. A., & Percle, G. A. (2000). Suicide among gay and lesbian adolescents and young adults: A review of the literature. Journal of Homosexuality, 40(1), 1–29.
Lasco, M., Jordan, T., Edgar, M., Petito, C., & Byrne, W. (2002). A lack of dimorphism of sex or sexual orientation in the human anterior commissure. Brain Research, 936(1/2), 95.
Laumann, E. O., Gagnon, J. H., Michael, R. T., & Michaels, S. (1994). The social organization of sexuality in the United States. Chicago, IL: University of Chicago Press.
Leitenberg, H., & Henning, K. (1995). Sexual fantasy. Psychological Bulletin, 117(3), 469–496.
Masters, W. H., & Johnson, V. E. (1966). Human sexual response. New York, NY: Bantam Books.
McQueeny, T., Schweinsburg, B., Schweinsburg, A., Jacobus, J., Bava, S., Frank, L.,…Tapert, S. F. (2009). Altered white matter integrity in adolescent binge drinkers. Alcoholism: Clinical & Experimental Research, 33(7), 1278–1285.
Meston, C. M., & Frohlich, P. F. (2000). The neurobiology of sexual function. Archives of General Psychiatry, 57(11), 1012–1030.
Miller, J., Naimi, T., Brewer, R., & Jones, S. (2007). Binge drinking and associated health risk behaviors among high school students. Pediatrics, 119(1), 76–85.
Miller, W. C. (1999). How effective are traditional dietary and exercise interventions for weight loss? Medicine & Science in Sports & Exercise, 31(8), 1129–1134.
Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2004). Actual causes of death in the United States, 2000. Journal of the American Medical Association, 291(10), 1238–1240.
Monteiro, M. (2001). A World Health Organization perspective on alcohol and illicit drug use and health. European Addiction Research, 7(3), 98–103.
Mustanski, B. S., Chivers, M. L., & Bailey, J. M. (2002). A critical review of recent biological research on human sexual orientation. Annual Review of Sex Research, 13, 89–140.
Nakazato, M., Murakami, N., Date, Y., Kojima, M., Matsuo, H., Kangawa, K., & Matsukura S. (2001). A role for ghrelin in the central regulation of feeding. Nature, 409(6817), 194–198.
Nestle, M., & Jacobson, M. F. (2000). Halting the obesity epidemic: A public health policy approach. Public Health Reports, 115(1), 12–24.
Norton, K. I., Olds, T. S., Olive, S., & Dank, S. (1996). Ken and Barbie at life size. Sex Roles, 34(3–4), 287–294.
Palmer B. (2008) Epidemiology, diagnosing and assessing eating disorders. Psychiatry, 7(4):143-146.
Patrick, L. (2002). Eating disorders: A review of the literature with emphasis on medical complications and clinical nutrition. Alternative Medicine Review, 7(3), 184–202.
Petersen, J. L., & Hyde, J. S. (2010). A meta-analytic review of research on gender differences in sexuality, 1993–2007. Psychological Bulletin, 136(1), 21–38.
Pillard, R., & Bailey, J. (1998). Human sexual orientation has a heritable component. Human Biology, 70(2), 347. Retrieved from Academic Search Premier Database.
Pillsworth, E., Haselton, M., & Buss, D. (2004). Ovulatory shifts in female sexual desire. Journal of Sex Research, 41(1), 55–65. Retrieved from Academic Search Premier Database.
Rahman, Q., & Wilson, G. D. (2003). Born gay? The psychobiology of human sexual orientation. Personality and Individual Differences, 34(8), 1337–1382.
Raj, A., Reed, E., Santana, M., Walley, A., Welles, S., Horsburgh, C.,…Silverman, J. G. (2009). The associations of binge alcohol use with HIV/STI risk and diagnosis among heterosexual African American men. Drug & Alcohol Dependence, 101(1/2), 101–106.
Rotermann, M. (2012). Sexual behaviour and condom use of 15- to 24-year olds in 2003 and 2009/2010 [PDF]. Statistics Canada, Catalogue no. 82-003-XPE. Health Reports, 23(1). Retrieved from http://www.statcan.gc.ca/pub/82-003-x/2012001/article/11632-eng.pdf
Rozin, P., Dow, S., Moscovitch, M., & Rajaram, S. (1998). What causes humans to begin and end a meal? A role for memory for what has been eaten, as evidenced by a study of multiple meal eating in amnesic patients. Psychological Science, 9(5), 392–396.in 2003 and
Saad, G., Eba, A., & Sejean, R. (2009). Sex differences when searching for a mate: A process-tracing approach. Journal of Behavioral Decision Making, 22(2), 171–190.
Schachter, S. (1968). Obesity and eating. Science, 161(3843), 751–756.
Schomer, H., & Drake, B. (2001). Physical activity and mental health. International SportMed Journal, 2(3), 1. Retrieved from Academic Search Premier Database.
Statistics Canada. (2010). Popularity of Physical Recreation Activities of Adults, Age 20+
(Canadian Community Health Survey). Available at: http://www.cflri.ca/eng/levels/popular_pa_adults.php. Accessed May 22, 2014.
Thornhill, R., & Gangestad, S. (1995). Human female orgasm and mate fluctuating asymmetry. Animal Behaviour, 50(6), 1601. Retrieved from Academic Search Premier Database.
Valencia-Martín, J., Galán, I., & Rodríguez-Artalejo, F. (2008). The joint association of average volume of alcohol and binge drinking with hazardous driving behaviour and traffic crashes. Addiction, 103(5), 749–757.
Vohs, K. D., Voelz, Z. R., Pettit, J. W., Bardone, A. M., Katz, J., Abramson, L. Y.,…Joiner, T. E., Jr. (2001). Perfectionism, body dissatisfaction, and self-esteem: An interactive model of bulimic symptom development. Journal of Social and Clinical Psychology, 20(4), 476–497.
West, S. L., D’Aloisio, A. A., Agans, R. P., Kalsbeek, W. D., Borisov, N. N., & Thorp, J. M. (2008). Prevalence of low sexual desire and hypoactive sexual desire disorder in a nationally representative sample of US women. Archives of Internal Medicine, 168(13), 1441–1449.
Williams, T., & Pepitone, M. (2000) Finger-length ratios and sexual orientation. Nature, 404, 455.
Wolf, G., & Miller, N. E. (1964). Lateral hypothalamic lesions: Effects on drinking elicited by carbachol in preoptic area and posterior hypothalamus. Science, 143(Whole No. 3606), 585–587.
World Health Organization. (2010). World Health Organization. Global Recommendations on Physical Activity for Health. Geneva, World Health Organization.
Yarema, M. (2013). Canada must respect the right to food. Huffington Post, Canada. Retrieved 2014 from http://www.huffingtonpost.ca/megan-yarema/olivier-de-schutter_b_2814600.html
Long Descriptions
| Biological influences: | Psychological influences: | Social-cultural influences: |
|---|---|---|
|
|
|
