
16.2 Stress and Coping
Jennifer Walinga
Learning Objectives
- Define coping and adaptation.
- Understand the various conceptualizations of stress as stimulus, response, and transactional process.
- Understand the role of cognition and physiology in coping with stress.
- Recognize emotion-focused and problem-focused coping strategies.
- Understand the relationships and interactions between health, stress, and coping.
In order to understand how people learn to cope with stress, it is important to first reflect on the different conceptualizations of stress and how the coping research has emerged alongside distinct approaches to stress. Stress has been viewed as a response, a stimulus, and a transaction. How an individual conceptualizes stress determines his or her response, adaptation, or coping strategies.
Stress As a Response
Stress as a response model, initially introduced by Hans Selye (1956), describes stress as a physiological response pattern and was captured within his general adaptation syndrome (GAS) model (Figure 16.3). This model describes stress as a dependent variable and includes three concepts:
- Stress is a defensive mechanism.
- Stress follows the three stages of alarm, resistance, and exhaustion.
- If the stress is prolonged or severe, it could result in diseases of adaptation or even death.
Later, in The Stress Concept: Past, Present and Future (1983), Selye introduced the idea that the stress response could result in positive or negative outcomes based on cognitive interpretations of the physical symptoms or physiological experience (Figure 16.3, “The General Adaptation to Stress Model“). In this way, stress could be experienced as eustress (positive) or dystress (negative). However, Selye always considered stress to be a physiologically based construct or response. Gradually, other researchers expanded the thinking on stress to include and involve psychological concepts earlier in the stress model.
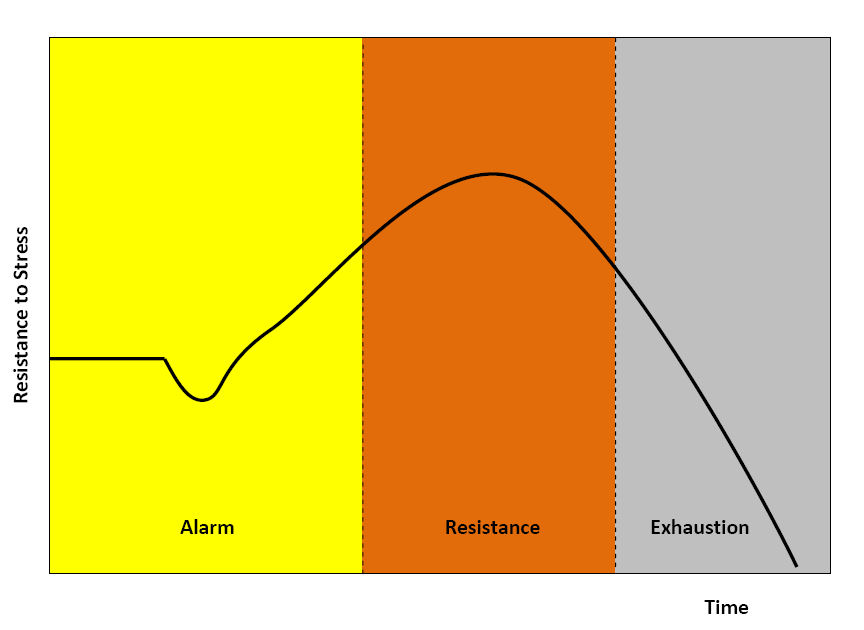
The response model of stress incorporates coping within the model itself. The idea of adaptation or coping is inherent to the GAS model at both the alarm and resistance stages. When confronted with a negative stimulus, the alarm response initiates the sympathetic nervous system to combat or avoid the stressor (i.e., increased heart rate, temperature, adrenaline, and glucose levels). The resistance response then initiates physiological systems with a fight or flight reaction to the stressor, returning the system to homeostasis, reducing harm, or more generally accommodating the stressor, which can lead to adaptive diseases such as sleep deprivation, mental illness, hypertension, or heart disease. Thus, along with the early conceptualization of stress as a physiological response, early research on coping was also born. As early as 1932, Walter Cannon described the notion of self-regulation in his work The Wisdom of the Body.
Stress As a Stimulus
The theory of stress as a stimulus was introduced in the 1960s, and viewed stress as a significant life event or change that demands response, adjustment, or adaptation. Holmes and Rahe (1967) created the Social Readjustment Rating Scale (SRRS) consisting of 42 life events scored according to the estimated degree of adjustment they would each demand of the person experiencing them (e.g., marriage, divorce, relocation, change or loss of job, loss of loved one). Holmes and Rahe theorized that stress was an independent variable in the health-stress-coping equation — the cause of an experience rather than the experience itself. While some correlations emerged between SRRS scores and illness (Rahe, Mahan, & Arthur, 1970; Johnson & Sarason, 1979), there were problems with the stress as stimulus theory. The stress as stimulus theory assumes:
- Change is inherently stressful.
- Life events demand the same levels of adjustment across the population.
- There is a common threshold of adjustment beyond which illness will result.
Rahe and Holmes initially viewed the human subject as a passive recipient of stress, one who played no role in determining the degree, intensity, or valence of the stressor. Later, Rahe introduced the concept of interpretation into his research (Rahe & Arthur, 1978), suggesting that a change or life event could be interpreted as a positive or negative experience based on cognitive and emotional factors. However, the stress as stimulus model still ignored important variables such as prior learning, environment, support networks, personality, and life experience.
Stress As a Transaction
In attempting to explain stress as more of a dynamic process, Richard Lazarus developed the transactional theory of stress and coping (TTSC) (Lazarus, 1966; Lazarus & Folkman, 1984), which presents stress as a product of a transaction between a person (including multiple systems: cognitive, physiological, affective, psychological, neurological) and his or her complex environment. Stress as a transaction was introduced with the most impact when Dr. Susan Kobasa first used the concept of hardiness (Kobasa, 1979). Hardiness refers to a pattern of personality characteristics that distinguishes people who remain healthy under life stress compared with those who develop health problems. In the late 1970s, the concept of hardiness was further developed by Salvatore Maddi, Kobasa, and their graduate students at the University of Chicago (Kobasa, 1982; Kobasa & Maddi, 1981; Kobasa, Maddi, & Kahn, 1982; Kobasa, Maddi, Puccetti, & Zola, 1985; Maddi & Kobasa, 1984). Hardiness has some notable similarities with other personality constructs in psychology, including locus of control (Rotter, 1966), sense of coherence (Antonovsky, 1987), self-efficacy (Bandura, 1997), and dispositional optimism (Scheier & Carver, 1985), all of which will be discussed in the next section. Researchers introduced multiple variables to the stress-as-transaction model, expanding and categorizing various factors to account for the complex systems involved in experiencing a stressor (Werner, 1993). The nature of stress was described in multiple ways: acute, episodic or intermittent, and chronic. Different types of stressors emerged, such as event, situation, cue, and condition, which then fell into categories based on locus of control, predictability, tone, impact, and duration. Figure 16.4 illustrates theories of stress as a response, stimulus, and transaction.

In his book Psychological Stress and the Coping Process (1966), Lazarus presented an elegant integration of previous research on stress, health, and coping that placed a person’s appraisal of a stressor at the centre of the stress experience. How an individual appraises a stressor determines how he or she copes with or responds to the stressor. Whether or not a stressor is experienced as discomforting is influenced by a variety of personal and contextual factors including capacities, skills and abilities, constraints, resources, and norms (Mechanic, 1978). Lazarus and Folkman (1984) unpacked the concept of interpretation further in their model of stress appraisal, which includes primary, secondary, and reappraisal components (see Figure 16.5, “The Transactional Theory of Stress and Coping”). Primary appraisal involves determining whether the stressor poses a threat. Secondary appraisal involves the individual’s evaluation of the resources or coping strategies at his or her disposal for addressing any perceived threats. The process of reappraisal is ongoing and involves continually reappraising both the nature of the stressor and the resources available for responding to the stressor.

Coping with Stress
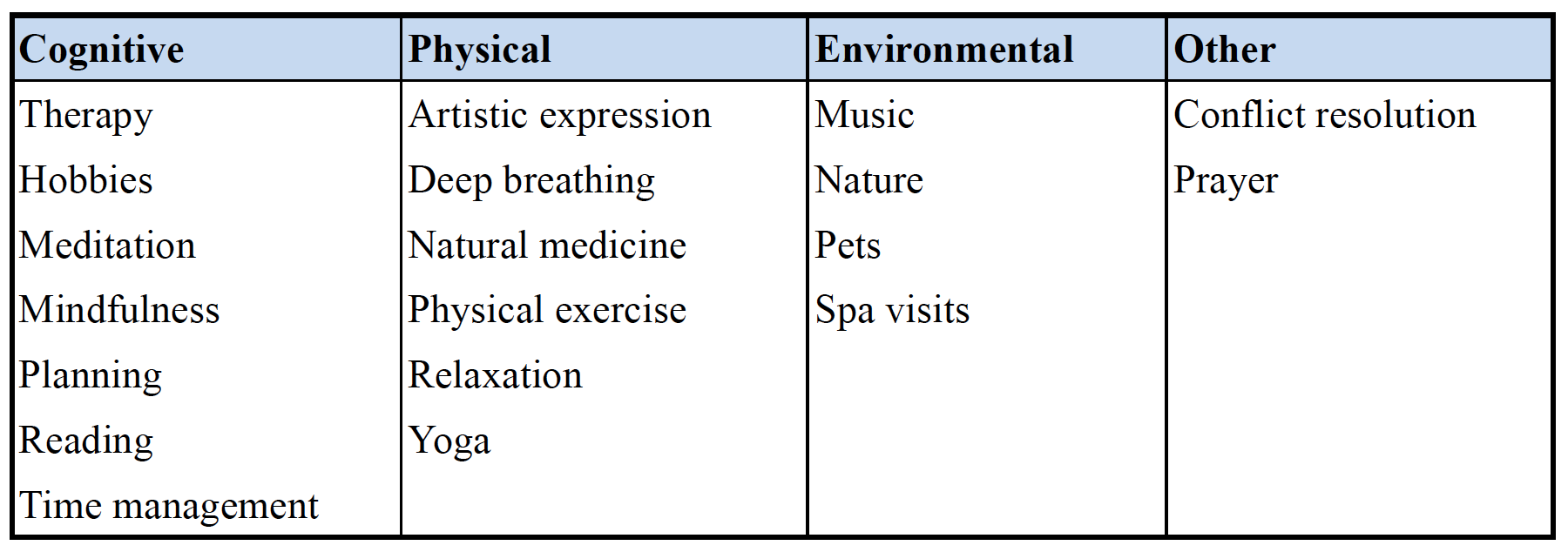
There are many ways that people strive to cope with stressors and feelings of stress in their lives. A host of literature, both popular and academic, extols the practice of stress management and whole industries are devoted to it. Many techniques are available to help individuals cope with the stresses that life brings. Some of the techniques listed in Figure 16.6, “Stress Management Techniques,” induce a lower than usual stress level temporarily to compensate the biological tissues involved; others face the stressor at a higher level of abstraction. Stress management techniques are more general and range from cognitive (mindfulness, cognitive therapy, meditation) to physical (yoga, art, natural medicine, deep breathing) to environmental (spa visits, music, pets, nature).
Stress coping, as described by researchers such as Lazarus and Folkman, implies a more specific process of cognitive appraisal to determine whether an individual believes he or she has the resources to respond effectively to the challenges of a stressor or change (Folkman & Lazarus, 1988; Lazarus & Folkman, 1987). The appraisal literature explains the response or coping process in terms of problem-focused coping or emotion-focused coping (Folkman & Lazarus, 1980; Lazarus & Folkman, 1984), also referred to as active and passive coping styles (Jex, Bliese, Buzzell, & Primeau, 2001). As well, approach and avoidance-style measures of coping exist involving assertiveness or withdrawal (Anshel, 1996; Anshel & Weinberg, 1999; Roth & Cohen, 1986). When faced with a challenge, an individual primarily appraises the challenge as either threatening or non-threatening, and secondarily in terms of whether he or she has the resources to respond to or cope with the challenge effectively. If the individual does not believe he or she has the capacity to respond to the challenge or feels a lack of control, he or she is most likely to turn to an emotion-focused coping response such as wishful thinking (e.g., I wish that I could change what is happening or how I feel), distancing (e.g., I’ll try to forget the whole thing), or emphasizing the positive (e.g., I’ll just look for the silver lining) (Lazarus & Folkman, 1987). If the person has the resources to manage the challenge, he or she will usually develop a problem-focused coping response such as analysis (e.g., I try to analyze the problem in order to understand it better; I’m making a plan of action and following it). It is theorized and empirically demonstrated that a person’s secondary appraisal then determines coping strategies (Lazarus & Folkman, 1987). Coping strategies vary from positive thinking to denial (see Figure 16.7, “COPE Inventory”) and are measured and tested using a variety of instruments and scales such as the COPE inventory (Carver, Scheier, & Weintraub, 1989).

Research Focus: Stress and Playing Soccer
Walinga (2008), in her work with a university soccer team that was undergoing several stressful changes in addition to the usual performance stressors, recently elaborated upon the appraisal model by suggesting that reappraisal more specifically involves a reiteration of the primary-secondary appraisal process. Once a person determines that a stressor is indeed a threat, and secondarily appraises resources as lacking, he or she then primarily appraises the secondary appraisal. In other words, the person determines whether having a lack of resources indeed poses some sort of threat. If lack of resources is deemed not to be a threat, the person is much more likely to generate creative solutions to the initial stressor and therefore cope effectively. But if a lack of resources is deemed to be a threat, then the person tends to focus on finding resources rather than addressing the initial stressor, and arrives at ineffective control-focused coping strategies.
In the case of the university soccer players, some initial stressors were identified as “a particularly challenging or sizable opponent,” “rainy conditions,” “the cold,” “not connecting with the coach,” or “negative attitudes on the field.” Typical emotion- or control-focused coping strategies included “working harder” and “sucking it up,” as well as avoidance or passivity. One player who struggled with her opponent’s size felt that she had little control over the fact that her opponent was taller and thus “beat her to the header balls.” She explained how she would “just kinda fade away when we play that team…get passive and just fade into the background.” Her coping response signified a withdrawal subscale on the emotion-focused coping scale, and when asked about her degree of satisfaction with her chosen path of response, she replied that she was “unhappy but could see no other alternative.” However, generally the team and several of the key leaders expressed alternative coping strategies not accounted for in the transactional theory of stress and coping. While several members of the team had a negative secondary appraisal, believing themselves to be lacking in the resources required to deal with the changes that occurred to the team, during the interviews it became apparent that such powerlessness did not, as was expected, lead only to emotion-focused coping, such as defensiveness, blame, or withdrawal; an acknowledged lack of control often resulted in an ability to move on and solve the challenges of change effectively.
Many of the team members believed “hitting rock bottom” accounted for their successful transformation, acting as a sort of “trigger” or “restart” and enabling them to gain greater clarity about their goals, as well as strategies for achieving these goals. Rather than focusing on increasing control or controlling the barrier or threat itself, the tolerant individual accepts the barrier as reality and accepts the lack of control as a reality. This person can now attend to and identify the challenges that the barrier poses to attaining her goals. For instance, the goalkeeper focused not on regretting or blaming herself for a missed save, or even trying harder next time, but instead focused on the challenges that a difficult shot posed for her and how she might resolve an unexpected spin on the ball. When faced with rainy conditions, the tolerant player focused not on denying or pushing through the rain, but on the problems the rain creates for her and how to resolve the resulting lack of ball control or slippery field conditions:
- “I guess the spin on the ball was out of my control, but I had total control in terms of adjusting to it.”
- “I was not in control of what my opponent did with the ball or could have done to ensure that I did not win the ball, but I was in control of making sure I did not dive into the tackle, I held my check up so we could get numbers back and avoid a counterattack.”
- “I went forward when I probably shouldn’t have and I left our defenders outnumbered in the back, so I made sure I won the ball so that we would not be faced with a 3-on-2.”
- “Despite my fatigue, I decided to make better decisions on when to commit myself and made sure I communicated when I needed help so that my opponent wouldn’t get a breakaway.”
- “The lights in my eyes were beyond my control, but I could control my focus on the ball and my positioning.”
- “I was not in control of the fact that they were fast; I was in control of my positioning and my decision making.”
By extending the theory of stress and coping, it is hypothesized here that when an individual perceives that he or she is lacking in resources to manage a threat, the perceived lack of control, and not necessarily anxiety, becomes the new challenge and focal point. If the person deems the perceived lack of control to be threatening or problematic for any reason, this would hypothetically cause him or her to fixate on increasing resources for managing the threat (control-focused coping), and impede any kind of response to the particular threats the challenge itself generates. If, on the other hand, the person accepts the lack of control, deeming the lack of resources to be a benign reality, he or she would be able to move the focus to the problems this threat creates and consider options for resolution and goal achievement (problem-focused coping). Control-focused coping seems to be a more generalizable construct for explaining an individual’s inability to focus on the problem at hand. The readiness model proposes that the appraisal process continues to cycle through the primary and secondary phases to determine an individual’s coping response (i.e., primary appraisal = Is it a threat?; secondary appraisal = Do I have the resources to change or control the threat?; if not, we find ourselves back at primary appraisal = Is my lack of control a threat?), and it is this cyclical process of appraisal that offers leverage for facilitating effective coping.
Related concepts to stress coping include locus of control (Rotter, 1966), sense of coherence (Antonovsky, 1987), self-efficacy (Bandura, 1997), and stress-related growth (Scheier & Carver, 1985). Rotter posited that a person with an internal locus of control believes that their achievements and outcomes are determined by their own decisions and efforts. If they do not succeed, they believe it is due to their own lack of effort. Whereas, a person with an external locus of control believes that achievements and outcomes are determined by fate, luck, or other. If the person does not succeed, he or she believes it is due to external forces outside of the person’s control. Aaron Antonovsky (1987) defined sense of coherence as:
a global orientation that expresses the extent to which one has a pervasive, enduring though dynamic feeling of confidence that (1) the stimuli deriving from one’s internal and external environments in the course of living are structured, predictable and explicable; (2) the resources are available to one to meet the demands posed by these stimuli; and (3) these demands are challenges, worthy of investment and engagement (pg. 19).
Self-efficacy is often confused with self-confidence, but in fact confidence is merely one of the many factors that make up a strong sense of self-efficacy. Albert Bandura (1997) defined self-efficacy as the extent or strength of one’s belief in one’s own ability to complete tasks and reach goals. Self-confidence is a trait measure (a quality that is built over time) whereas self-efficacy is a state measure (a capacity experienced at a specific point in time and concerning a specific task). Stress-related growth or thriving is a dispositional response to stress that enables the individual to see opportunities for growth as opposed to threat or debilitation. Spreitzer and colleagues (2005) offered a preliminary definition of thriving as a “psychological state in which individuals experience both a sense of vitality and a sense of learning at work” (p. 538). Carver (1998) described thriving as being “better off after adversity” (p. 247). There are many examples of individuals surpassing previous performances when faced with particularly stressful scenarios, showing increased growth and strength in the face of adversity.
Coping and Health
The capacity for thriving, resilience, or stress-related growth has been associated with improved health outcomes. For example, building on Carver’s work on dispositional optimism and thriving, Shepperd, Maroto, and Pbert (1996) found, in their longitudinal study of cardiac patients, that optimism predicts success in making health changes associated with lower risk of cardiac disease. Optimism was significantly and directly correlated with improved health outcomes, including lower levels of saturated fat, body fat, and global coronary risk, and positively associated with success in increasing aerobic capacity. Billings and colleagues (2000) showed that coping affected positive and negative affect among men who were caregiving for AIDS patients. Social support coping predicted increases in positive affect, which in turn were related to fewer physical symptoms. Avoidant coping, however, was related to increases in negative affect, which were related to more physical symptoms.
Research Focus: Coping with Melanoma
Perhaps the most dramatic of stress coping interventions studies was conducted by Fawzy and his colleagues (Fawzy, Cousins, Fawzy, Kemeny, & Morton, 1990; Fawzy, Kemeny, et al., 1990; Fawzy, et al., 1993; Fawzy & Fawzy, 1994), who did specific coping skills interventions with melanoma patients. During a six-week structured program, participants experienced multiple program components including health education, psychological support, problem-solving, and stress management training. In the short term, the experimental subjects were more likely to use active behaviour coping than the controls, and also had more positive affect. Differences in immune functioning were evident between the two groups at the six-month assessment. Specifically, experimental subjects had a greater percentage of large granular lymphocytes, more NK cells, and better NK cytotoxicity. While coping strategies were not directly associated with immune cell changes, they were correlated with affect, which in turn was associated with immune functioning. The studies supported the hypothesis that effects of coping on biomedical outcomes may be mediated through affect. At a five-year follow-up, a third of the control group had died, compared with less than 10% of the experimental group. Longer survival was associated with more active coping at baseline.
Key Takeaways
- Stress has been conceived of in different ways: as a response, as a stimulus, and as a transaction.
- Stress as response treats stress as the physiological dependent variable.
- Stress as stimulus treats stress as a life event or change that acts as an independent variable.
- Stress as transaction considers the myriad personal, social, and environmental factors that come into play in determining the nature, degree, and impact of the stress experience.
- There are a variety of stress management techniques deriving from a multitude of theoretical derivations and philosophies.
- Coping with stress can be a trait or state-based process — an inherent quality or ability or a learned skill or capacity.
- How people appraise a stressor determines how they will attempt to cope with the stressor.
- Appraisal hinges on multiple human, social, and environmental factors.
- Concepts related to coping include optimism, thriving, hardiness, locus of control, and self-efficacy, all qualities and capacities that can influence the coping strategies an individual chooses to apply to a stressor.
Exercises and Critical Thinking
- Reflect on a recent emotionally or physiologically impactful stressor that you perceived to be threatening or negative. What social, environmental, and personal factors contributed to your appraisal of the stressor? Referencing the list of coping items on the COPE inventory, what types of coping strategies did you apply?
- Imagine a stressful situation that you believe you coped with positively. Can you identify some coping strategies you used? Can you determine whether you were able to grow through the experience? What factors facilitated a positive outcome for you?
- What are some major life events you have experienced? Can you identify differences in how you appraised these events? How you coped with these events?
References
Anshel, M.H. (1996). Coping styles among adolescent competitive athletes. The Journal of Social Psychology, 136, 311-323.
Anshel, M.H. & Weinberg, R.T. (1999). Re-examining coping among basketball referees following stressful events: Implications for coping interventions. Journal of Sport Behavior, 22, 144-161.
Antonovsky, A. (1987). Unraveling the mystery of health: How people manage stress and stay well. San Francisco: Jossey Bass.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman.
Billings, D. W., Folkman, S., Acree, M., & Moskowitz, J. T. (2000). Coping and physical health during caregiving: The roles of positive and negative affect. Journal of Personality and Social Psychology, 79, 131–142.
Carver, C. S. (1998). Resilience and thriving: Issues, models, and linkages. Journal of Social Issues, 54, 245–266.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56, 267–283.
Cannon, W. B. (1932). The Wisdom of the Body. New York: W.W. Norton.
Fawzy, F., & Fawzy, N. (1994). Psychoeducational interventions and health outcomes. In R. Glaser and J. K. Kiecolt-Glaser (Eds.). Handbook of human stress and immunity (pp. 365–402). San Diego: Academic Press.
Fawzy, F. I., Fawzy, N. W., Hyun, C., Elashoff, R., Guthrie, D., Fahey, J. L., & Moron, D. L. (1993). Malignant melanoma: Effects on early structured psychiatric intervention, coping, and affective state on recurrence and survival six years later. Archives of General Psychiatry, 50, 681–689.
Fawzy, F. I., Cousins, N., Fawzy, N. W., Kemeny, M., & Morton, D. I. (1990). A structured psychiatric intervention for cancer patients: I. Changes over time in methods of coping and affective disturbance. Archives of General Psychiatry, 47, 720–725.
Fawzy, F. I., Kemeny, M., Fawzy, N. W., Elashoff, R., Morton, D., Cousins, N., & Fahey, J. L. (1990). A structured psychiatric intervention for cancer patients: II. Changes over time in immunological measures. Archives of General Psychiatry, 47, 729–235.
Folkman, S. & Lazarus, R.S. (1980). An analysis of coping in a middle-aged community sample. Journal of Health & Social Behavior, 21(3), 219-239.
Folkman, S., Lazarus, R. S. (1988). Coping as a mediator of emotion. Journal of Personal and Social Psycholog,. 54, 466-75.
Holmes, T., & Rahe, R. (1967). The Social Reajustment Rating Scale. Journal of Psychosomatic Research, 12,(4), p. 213–233.
Jex, S.M., Bliese, P.D., Buzzell, S., & Primeau. J. (2001). The impact of self-efficacy on stressor–strain relations: Coping style as an explanatory mechanism. Journal of Applied Psychology 86 (3), 401.
Johnson , J. H., & Sarason , I. G. (1979). Moderator variables in life stress research. In I. Sarason & C. Spielberger (Eds.), Stress and anxiety, 6, 151–167.
Kobasa, S. C. (1979). Stressful life events, personality, and health – Inquiry into hardiness. Journal of Personality and Social Psychology, 37(1), 1–11.
Kobasa, S. C. (1982). The hardy personality: Toward a social psychology of stress and health. In G. Sanders & J. Suls (Eds), social Psychology of Health and Illness (p. 3-32). Hillsdale, NJ: Erlbaum.
Kobasa, S. C., Maddi, S. R., & Courington, S. (1981). Personality and constitution as mediators in the stress-illness relationship. Journal of Health and Social Behavior 22(4), 368–378.
Kobasa, S. C., Maddi, S. R., & Kahn, S. (1982). Hardiness and health: A prospective study. Journal of Personality and Social Psychology 42(1), 168–177.
Kobasa, S. C., Maddi, S. R., Puccetti, M. C., & Zola, M. A. (1985). Effectiveness of hardiness, exercise and social support as resources against illness. Journal of Psychosomatic Research 29(5), 525–533.
Lazarus, R. S. (1966). Psychological stress and the coping process. New York, NY: McGraw-Hill.
Lazarus, R. S. (1999). Stress and emotion: A new synthesis. New York: Springer.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
Lazarus, R. S., & Folkman, S. (1987). Transactional theory and research on emotions and coping. European Journal of Personality, 1, 141–169.
Maddi, S. R., & Kobasa, S. C. (1984). The hardy executive: Health under stress. Homewood, IL: Dow Jones-Irwin.
Mechanic, D. (1978). Students under stress: A study in the social psychology of adaptation. Madison: University of Wisconsin Press.
Rahe, R. H., & Arthur, R. J. (1978). Life change and illness studies: Past history and future directions. Journal of Human Stress, 4, 3–15.
Rahe R. H., Mahan J. L., & Arthur R. J. (1970). Prediction of near-future health change from subjects’ preceding life changes. Journal of Psychosomatic Research, 14(4), 401–6.
Roth, S., & Cohen, L.J. (1986). Approach, avoidance, and coping with stress. American Psychologist, 41, 813-819.
Rotter, J. B. (1966) Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80 Sanders, G.S. & Suls, J. (Eds.), Social psychology of health and illness (pp. 1–25).
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health – Assessment and implications of generalized outcome expectancies. Health Psychology, 4(3), 219–247.
Selye, H. (1956). The stress of life. New York: McGraw Hill.
Selye, H. (1983). The concept of stress: Past, present and future. In C.L. Cooper (Ed.). Stress research: Issues for the eighties. New York: John Wiley.
Shepperd, J. A., Maroto, J. J., & Pbert , L. A. (1996). Dispositional optimism as a predictor of health changes among cardiac patients. Journal of Research in Personality 30, 517–534.
Spreitzer, G., Sutcliffe, K., Dutton, J., Sonenshein, S. & Grant, A. (2005). A socially embedded model of thriving at work. Organization Science 16(5): 537-549.
Walinga, J. (2008). Change Readiness: The Roles of Appraisal, Focus, and Perceived Control. Journal of Applied Behavioral Science, 44(3), 315–347.
Werner, E.E. (1993). Risk, resilience, and recovery: Perspectives from the Kauai longitudinal study. Development and Psychopathology, 5, 503-515.
Image Attributions
Figure 16.3: A diagram of the General Adaptation syndrome model by David G. Myers (http://commons.wikimedia.org/wiki/File:General_Adaptation_Syndrome.jpg) used under the CC-BY 3.0 (http://creativecommons.org/licenses/by/3.0/deed.en).
Figure 16.4: by J. Walinga.
Figure 16.5: by J. Walinga.
Figure 16.6: by J. Walinga.
Figure 16.7: Adapted by J. Walinga from Carver, Scheier, & Weintraub, 1989.
Long Descriptions
| Cognitive | Physical | Environmental | Other |
|---|---|---|---|
|
|
|
|
[Return to Figure 16.6]
Figure 16.7 long description: COPE Inventory scale of coping techniques
- positive reinterpretation and growth
- mental disengagement
- focus on and venting of emotions
- use of instrumental social support
- active coping
- denial
- religious coping
- humour
- behavioural disengagement
- restraint
- use of emotional social support
- substance use
- acceptance
- suppression of competing activities
- planning
