
Sarcopenia and Frailty
Learning Objectives
Why the development of frailty impacts quality of life and longevity.
- Sarcopenia is the driving force for frailty.
- The development and progression of frailty is a dynamic process.
- Progressing frailty is connected to an array of geriatric symptoms.
The Development of Frailty Impacts Quality of Life And Longevity
What are you picturing when I talk about a frail person? Most likely, you think of a very thin and delicate person that could be blown over by a strong wind. This is not necessarily the case.
Frailty can come with thinness or obesity. The main descriptor is having little strength and a decreased ability to cope with everyday stressors. Frail people are vulnerable for disability, diseases, physical and cognitive impairments and geriatric diseases such as falls, delirium and urinary incontinence. In fact, today we see an early onset of frailty—particularly in obese people living a sedentary lifestyle—and especially if they have developed chronic diseases.
The driving force behind frailty is sarcopenia, independent of weight.
Risk Factors Factors for Developing Sarcopenia

People can develop frailty at any point during their life. In younger people this is usually due to disease. Several risk factors that come with aging accelerate the risk for frailty.
A sedentary lifestyle leads to loss of muscle mass leading to a loss of strength over time. This is aggravated by age-associated anatomical changes leading to a remodeling of the muscle motor unit.
The anatomical changes limit communication between neuron and muscle fiber reducing the functionality of the muscle. Loss of muscle mass accelerates especially when the person leads a sedentary lifestyle.
In high age metabolic changes make it harder to gain and maintain muscle. Protein synthesis becomes more inefficient (for example ER stress increases misfolding of proteins, chapter 30) and anabolic signals promoting muscle growth after physical activity such as growth hormone, IGF, testosterone and thyroid hormones decline.
Elderly people do not just lose muscle mass, they also see an increase in ectopic fat. Ectopic fat infiltrates muscles fiber and reduces muscle functionality and strength.
Increased inflammation changes muscle cell function and mitochondrial dysfunction (chapter 30) reduces available ATP in the muscle cell. The elderly person has less energy to be active, tires faster and becomes more sedentary.
These aging-associated processes increase the vulnerability for sarcopenia by themselves. In addition, obesity and chronic diseases accelerate those processes and people can develop sarcopenia earlier in life.
How to Diagnose Sarcopenia

For the longest time, sarcopenia was defined as the loss of muscle mass due to inactivity or old age. However, recent studies did not find a direct connection between low muscle mass, disability, and mortality. Instead, those newer studies found a connection to disability, morbidity, cognitive decline, and lower survival times when both physical performance and muscle strength were impaired.
This led to a new definition of sarcopenia as low muscle mass combined with either low muscle strength and/or low physical performance.
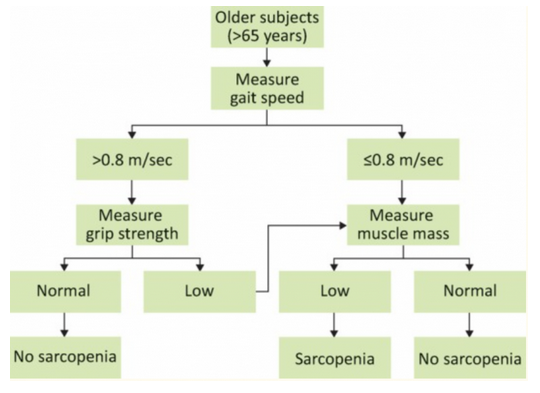
It is important to know the signs of and/or get tested for sarcopenia development. The European Working Group on Sarcopenia for Older People (EWGSOP) has developed standards for diagnostic testing, which is recommended for individuals aged 65 and older, across three parameters:
- Physical performance: This is usually the first test conducted and is done so by observing patient gait speed (walking speed). The standard for a normal gait speed is anything greater than 0.8 meters per second. The gait speed can be measured in a hallway and requires only a measuring tape and some masking tape to mark start and end points. The patient has 2 meters to accelerate, then walks between 4 and 10 meters at top speed. This stretch is timed and the gait speed calculated.
- Muscle Strength: This is tested through the use of a hand grip called a Dynamometer. Squeezing the grip will display the amount of strength in kilograms with the normal being about 28.0-44.0 kg and 15.0-27.0 kg for males and females respectively.
- Muscle Mass: This is usually the last test conducted, and is most commonly done through dual-energy X-ray absorptiometry (DXA). Among other mass tests, it is the most accurate at estimating the proportion of lean mass, fat, and bone density. The skeletal mass is divided by the individuals height to determine the amount of mass, while cut-offs are based on individual factors.
The final diagnosis of sarcopenia is done through a combination of these tests.
Prevention and Treatment of Sarcopenia
The best way to prevent sarcopenia is a having a healthy lifestyle in young and middle adulthood. It is similar to osteoporosis, in that developing optimal bone density will give you a reserve when bone loss naturally occurs during aging. Developing a healthy level of lean body mass and muscular strength will give you a reserve during age-related LBM decline.
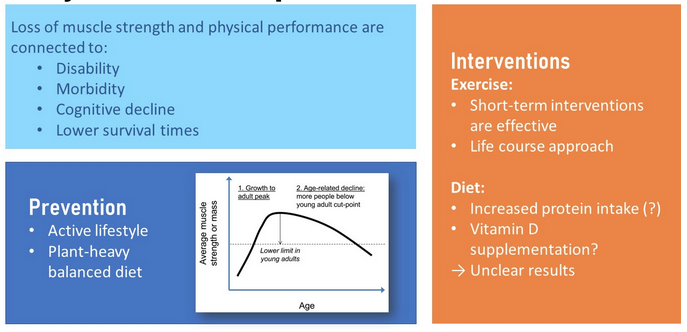
Does that mean that nothing can be done if sarcopenia develops with age? Here the research is promising. Short-term exercise interventions, including resistance training (about 5 months), have been effective in increasing quality of life and independence. Dietary interventions such as protein and vitamin D supplementation are researched as well, but with unclear results.
Sarcopenia Is the Driving Factor For Frailty
Failure to diagnose and effectively treat sarcopenia will inevitably lead to a state of frailty. When thinking of frailty, the word “fragile” comes to mind. If not handled with care, fragile objects can break/fall apart. While I hope you’re not picking up elderly people and dropping them, someone experiencing frailty must be handled and treated with the utmost care, otherwise a cascading decline across multiple dimensions of health will begin.
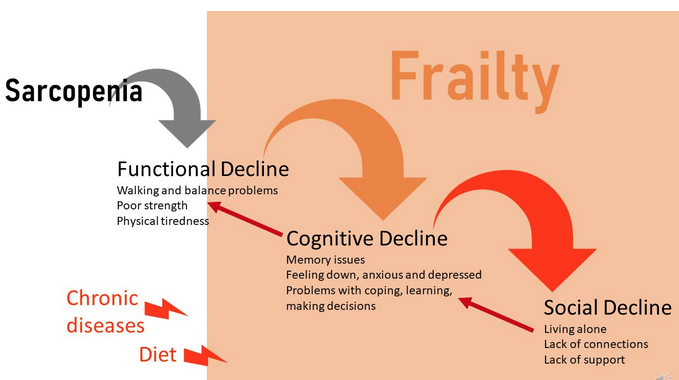
Sarcopenia leads first to a functional decline. Once people cross a certain sarcopenia threshold, poor strength and physical tiredness leads to walking and balancing problems. After developing these problems, people with sarcopenia go out less often and spend more time at home, eventually limiting physical activity entirely. Frailty sets in.
A life once full of activity and social interaction completely changes; as frail people begin spending more time alone, they tend to feel down, anxious, and depressed. Mitochondrial dysfunction also affects the brain which leads to problems with coping, learning, and making decisions.
Social isolation due to the inability to move and the avoidance of challenging situations will lead to social decline.
The three areas of frailty—functional, social and cognitive decline—are not isolated from each other. Social isolation leads to less stimulation which hastens the cognitive decline. Feeling bored and alone increase depression symptoms. Depression and social isolation leads to less movement because there is no reason to challenge oneself.
You can clearly see how sarcopenia, once it results in frailty, can start a vicious downward spiral.
The Development and Progression of Frailty Is a Dynamic Process
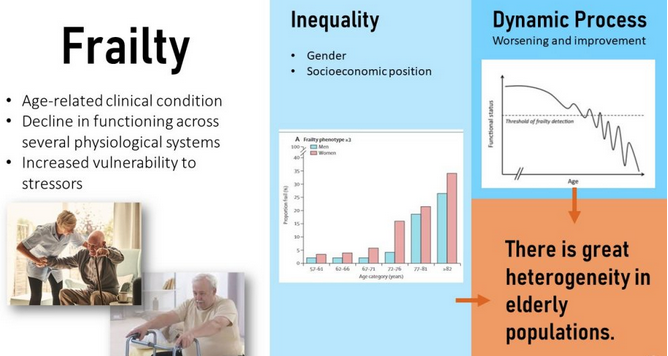
Frailty is an age-related clinical condition connected to a decline in functioning across several physiological systems, as well as an increased vulnerability to stressors. Frailty is not a straight line to death, rather the condition oscillates up and down until frailty spirals out of control and hastens death.
“The interconnected nature of frailty can lead to substantial declines across multiple forms of well-being. When I worked in a retirement home, multiple forms of frailty could be visibly seen in the residents. From a displeased scowl directed at the nights dinner to a resident socially isolating themselves in the corner of the dining room, it was easy to see these forms of frailty unfold.
However, there were times when the socially isolated resident would meander over to a small table of three and engaged in small talk. I even walked into the four of them blissfully devouring dairy queen together, a interaction so humbling that branding the resident as isolated would have never have come to mind.
This example actually represents the dynamic nature of frailty. It’s not a simple linear decline towards dysfunctionality, but rather a wellbeing water slide with twists and turns that make some days great and others not so much.
What separates the bad from the good days is usually the amount of stressors someone with frailty faces. Being in the declined state that they are, even the smallest forms of stress can have a huge impact. Waking up to find that the cereal, a routine order for one of my residents, was accidentally misplaced with a fruit bowl was too much for this resident to handle and it sent them into spiraling rage for the next few days.
This dynamic, if not handled with care, will eventually lead to a dangerous state of frailty that contributes to health risks. Those most immediate risks include falls, delirium, and fluctuating disability. This inevitably leads to increases healthcare costs and can force some families to make the decision to admit an elderly relative to long-term care facilities or hospitals.” ~ Eric
Frailty is not equally distributed in our society. Women are more affected than men, and the more financial resources a person has, the less the aging process is connected with frailty. People with a low income cannot afford to live in an environment with ample social stimulation, a variety of exercise, or eating a healthy diet. Once frail seniors need to give up their home environment and live in a care facility, money determines their ability to live in an environment that offers cognitive and social stimulation, as well as exercise classes.
Progressing Frailty Is Connected to an Array of Geriatric Symptoms
When sarcopenia reaches a threshold, the first symptoms of frailty show. The first symptom is usually undue exhaustion as daily living starts to cause excessive fatigue. Consequently, the person slows down and eventually lowers physical activity entirely. The reduced physical activity leads to more muscle loss, and general weakness sets in.

Once frailty takes hold and continues to progress, other feared geriatric symptoms can be detected, including cognitive decline, decreased strength, and balance problems. These symptoms often lead to increased instances of falls—resulting in broken bones and injuries—which further reduces physical activity and leads to an accelerated cognitive decline. Once the frail person spends most of the day in bed, pressure ulcers and delirium are feared.
In clinical settings, the clinical frailty scale (to the right in above graphic) is used to identify the degree of frailty and start appropriate interventions.
Keep in mind that people can cope very differently, and therefore the trajectory of frailty is very individual. A person that is still socially connected with plenty of family and friends will cope with a setback (for example, from a fall) easier and recuperate. Or not, if the frail person is more depressed or anxious by nature. The living environment plays a huge role here; meaningful social connections, cognitive stimulation, and continued exercising will keep the person on a much slower trajectory.
Frailty Prevention and Intervention Strategies Include Diet and Exercise

Because frailty can be present in normal weight, overweight, or obese individuals, sudden weight loss is the best predictor for sarcopenia, developing frailty, and ultimately mortality. Spotting the sudden weight loss and starting lifestyle interventions can prolong life and increase quality of life.
The available knowledge for the effectiveness of nutrition intervention is limited, and no “perfect blueprint” has been found. Despite this, suggested dietary interventions generally prioritize reducing severe obesity for both easier physical activity and reduced inflammation. Generally, these goals are supported by eating a plant-heavy diet rich in antioxidants and flavonoids. At the moment, the recommended diet is a Mediterranean-style diet because studies have demonstrated a positive impact on inflammation, chronic diseases, and cognition. Because not all elderly people will accept a Mediterranean diet, similar culturally-appropriate diets such as the DASH diet are good choices as well.
The main goal of the dietary intervention is to prevent sudden weight loss, especially from muscle mass. Research has focused heavily on increased protein intake, vitamin D, omega-3 fatty acids, and antioxidant supplementation as intervention strategies. Although clinical trials have shown mixed results, the intake for these nutrients should be adequate to support maintenance of muscle mass and build reserves.
As always, prevention is better than intervention. A healthy, plant-based diet will be the first important preventative step to avoid sarcopenia and frailty. A focus on protein intake is more important once people reach old age, since most Americans have an over-adequate protein intake.
Image Credits
- Welch, G., Schwartz, L., Woloshin S. (2005). The exaggerated relations between diet, body weight and mortality: the case for a categorical data approach. CMAJ 172 (7). DOI: https://doi.org/10.1503/cmaj.1041310
- Kuk JL, Saunders TJ, Davidson LE, Ross R. Age-related changes in total and regional fat distribution. Ageing Res Rev. 2009;8(4):339–348. doi: 10.1016/j.arr.2009.06.001.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31. doi: 10.1093/ageing/afy169.
Chapter Attribution
Chapter 31 Obesity, Sarcopenia, and Frailty Prevent Longevity by Sabine Zempleni and Eric Hanzel in Nutrition Through the Lifecycle, published by the University of Nebraska under a CC BY-NC-ND license. Used with permission.
Basic functional unit of the skeletal muscle comprised of the motoneuron and the muscle fiber innervated
