
Our large, complex bodies need blood to deliver nutrients to and remove wastes from our trillions of cells. The heart, as discussed in the previous chapter, pumps blood throughout the body in a network of blood vessels. Together, these three components—blood, heart, and vessels—makes up the cardiovascular system.
Virtually every cell, tissue, organ, and system in the body is impacted by the circulatory system. This includes the generalized and more specialized functions of transport of materials, capillary exchange, maintaining health by transporting white blood cells and various immunoglobulins (antibodies), hemostasis, regulation of body temperature, and helping to maintain acid-base balance. Table 13.1 summarizes the important relationships between the circulatory system and the other body systems.
| SYSTEM | ROLE OF CIRCULATORY SYSTEM |
Digestive
 |
Absorbs nutrients and water; delivers nutrients (except most lipids) to liver for processing by hepatic portal vein; provides nutrients essential for hematopoiesis and building hemoglobin. |
Endocrine
 |
Delivers hormones: atrial natriuretic hormone (peptide) secreted by the heart atrial cells to help regulate blood volumes and pressures; epinephrine, ANH, angiotensin II, ADH, and thyroixine to help regulate blood pressure; estrogen to promote vascular health in women and men. |
Integumentary
 |
Carries clotting factors, platelets, and white blood cells for hemostasis, fighting infection, and repairing damage; regulates temperature by controlling blood flow to the surface, where heat can be dissipated; provides some coloration of integument; acts as a blood reservoir. |
Lymphatic
 |
Transports various white blood cells, including those produced by lymphatic tissue, and immunoglobulins (antibodies) throughout the body to maintain health; carries excess tissue fluid not able to be reabsorbed by the vascular capillaries back to the lymphatic system for processing. |
Muscular
 |
Provides nutrients and oxygen for contraction; removes lactic acid and distributes heat generated by contraction; muscular pumps aid in venous return; exercise contributes to cardiovascular health and helps to prevent atherosclerosis. |
Nervous
 |
Produces cerebrospinal fluid (CSF) within choroid plexuses;contributes to blood-brain barrier; cardiac and vasomotor centers regulate cardiac output and blood flow through vessels via the autonomic system. |
Reproductive
 |
Aids in erection of genitalia in both sexes during sexual arousal; transports gonadotropic hormones that regulate reproductive functions. |
Respiratory
 |
Provides blood for critical exchange of gases to carry oxygen needed for metabolic reactions and carbon dioxide generated as byproducts of these processes. |
Skeletal
 |
Provides calcium,phosphate, and other minerals critical for bone matrix; transports hormones regulating buildup and absorption of matrix including growth hormone (somatotropin), thyroid hormone, calcitronins, and parathryoid hormones; erythropoietin stimulates myeloid cell hematopoiesis; some level of protection for select vessels by bony structures. |
Urinary
 |
Delivers 20% of resting circulation to kidneys for filtering, reabsorption of useful products, and secretion of excesses; regulates blood volume and pressure by regulating fluid loss in the form of urine and by releasing the enzyme renin that is essential in the renin-angiotensin-aldosterone mechanism. |
Watch this video:
Media 13.1 Blood Vessels, Part 1 – Form and Function: Crash Course A&P #27 [Online video]. Copyright 2015 by CrashCourse.
Cardiovascular System – Blood Vessels and Blood Medical Terms
Anatomy of the Blood Vessels
Blood pumped by the heart flows through a series of vessels known as arteries, arterioles, capillaries, venules, and veins before returning to the heart.
- Arteries transport blood away from the heart and branch into smaller vessels, forming arterioles.
- Arterioles distribute blood to capillary beds, the sites of exchange with the body tissues.
- A capillary is a microscopic channel that supplies blood to the tissues themselves, a process called perfusion.
- Exchange of gases and other substances occurs in the capillaries between the blood and the surrounding cells and their tissue fluid (interstitial fluid).
- For capillaries to function, their walls must be leaky, allowing substances to pass through.
- Capillaries lead back to small vessels known as venules.
- Venules are small veins that converge into larger veins.
- A vein is a blood vessel that conducts blood toward the heart
- Compared to arteries, veins are thin-walled vessels with large and irregular lumens
- Larger veins are commonly equipped with valves that promote the unidirectional flow of blood toward the heart and prevent backflow toward the capillaries caused by the inherent low blood pressure in veins as well as the pull of gravity
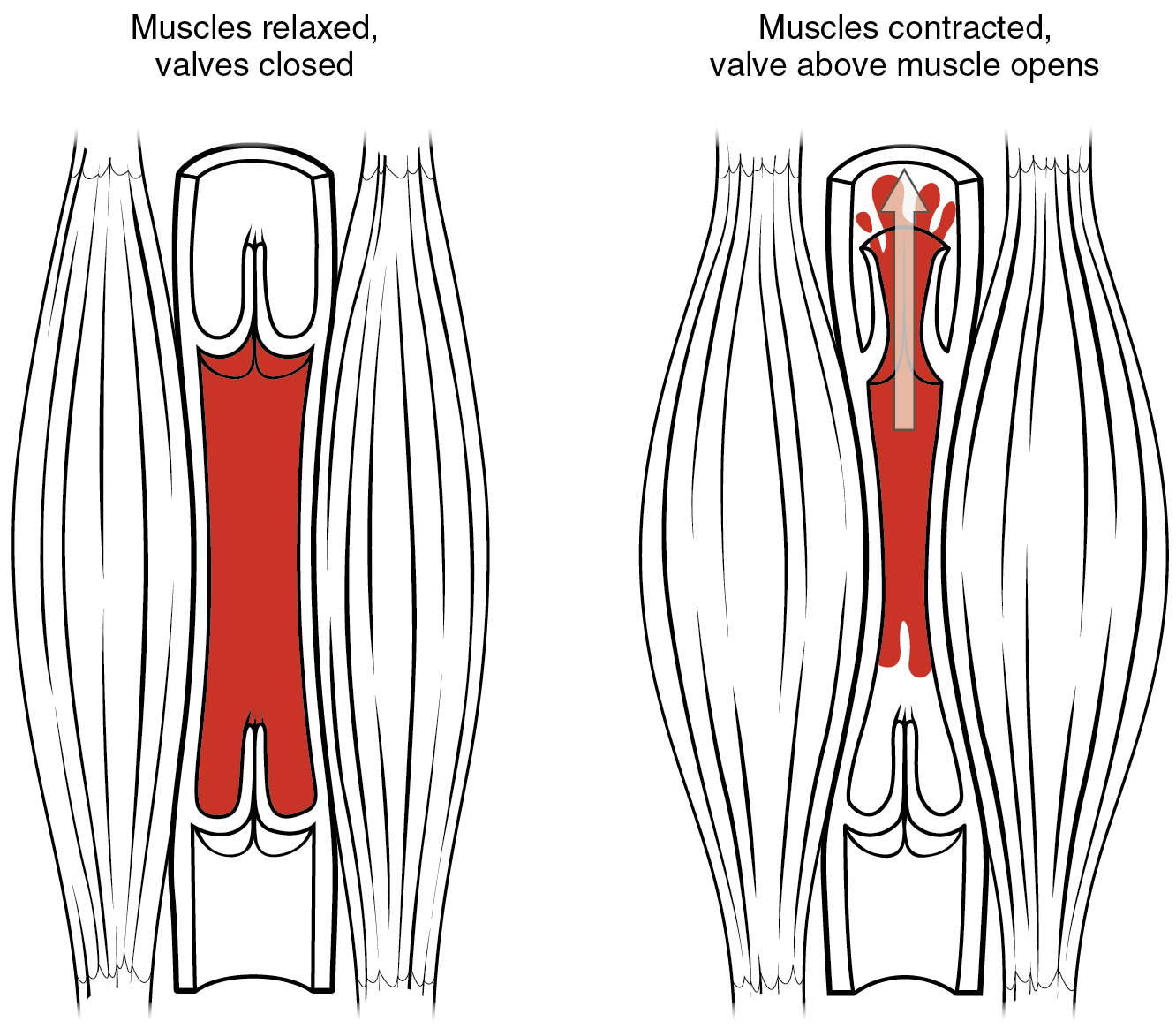
- Other ways in which the body assists the transport of venous blood back to the heart involve contractions of skeletal muscles in the extremities (see figure below), as well as pressure variations caused by breathing motion in the chest.
Concept Check
- Select the correct bolded word: Arteries always carry blood away from/towards the heart
- Select the correct bolded word: Veins always carry blood Away from/towards the heart.
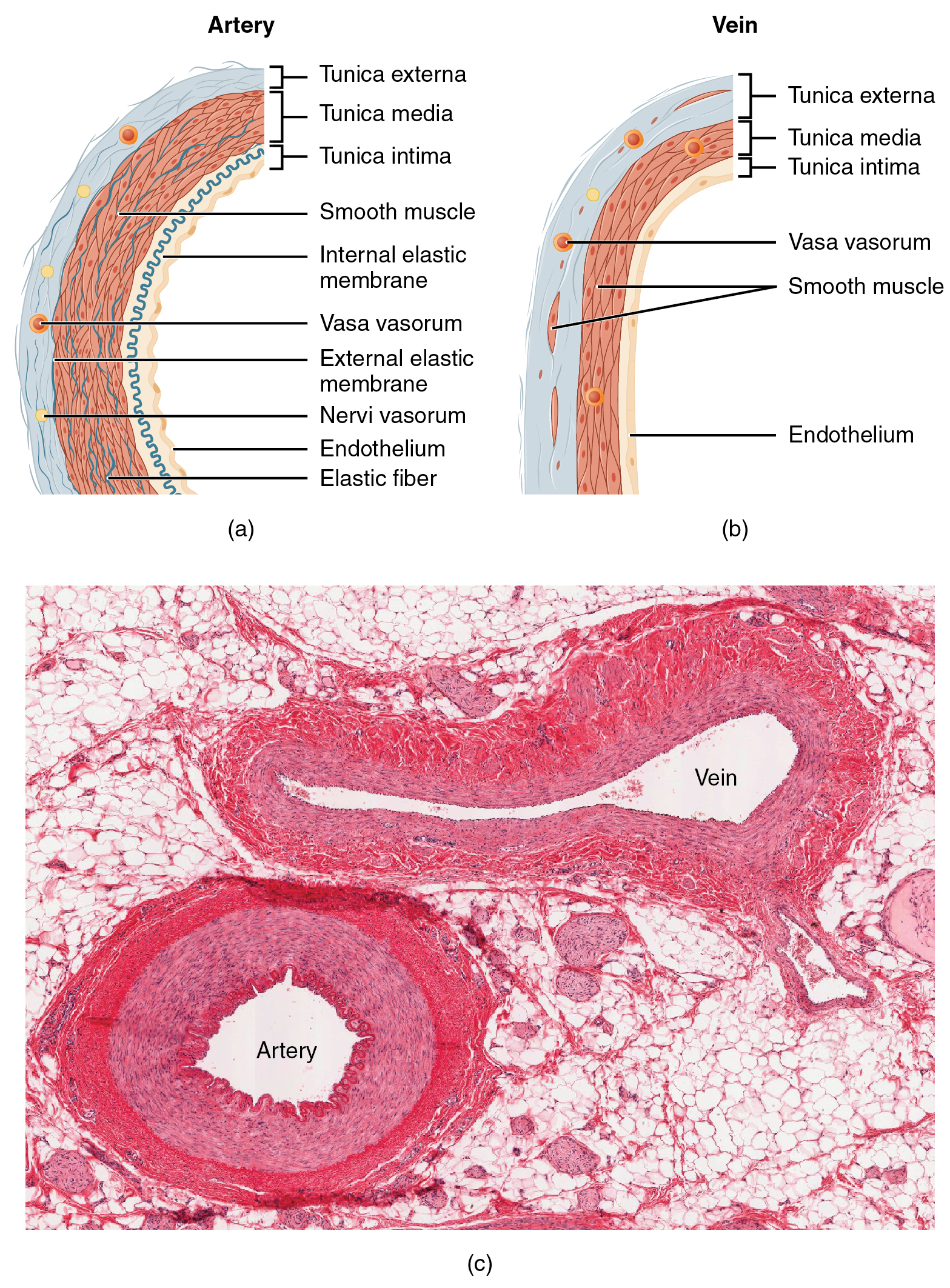
Both arteries and veins have the same three distinct tissue layers, called tunics, for the garments first worn by ancient Romans. From the most interior layer to the outer, these tunics are the tunica intima, the tunica media, and the tunica externa (see Figure 13.3). The smooth muscle in the middle layer, the tunica media, provides the vessel with the ability to vasoconstrict and vasodilate as needed to ensure sufficient blood flow.
| CHARACTERISTIC | ARTERIES | VEINS |
|---|---|---|
| Direction of blood flow | Conducts blood away from the heart | Conducts blood toward the heart |
| General appearance | Rounded | Irregular, often collapsed |
| Pressure | High | Low |
| Wall thickness | Thick | Thin |
| Relative oxygen concentration | Higher in systemic arteries
Lower in pulmonary arteries |
Lower in systemic veins
Higher in pulmonary veins |
| Valves | Not present | Present most commonly in limbs and in veins inferior to the heart |
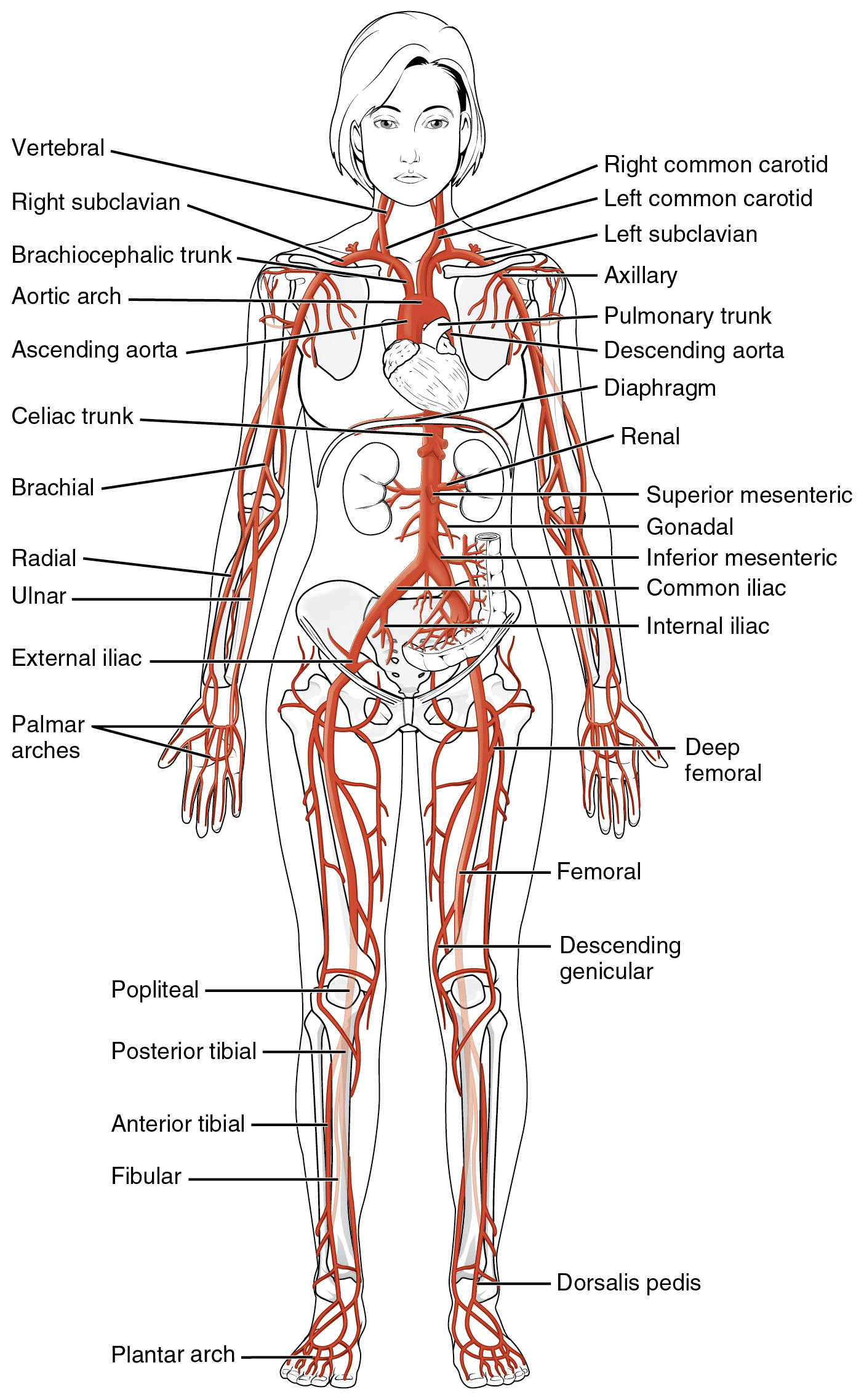
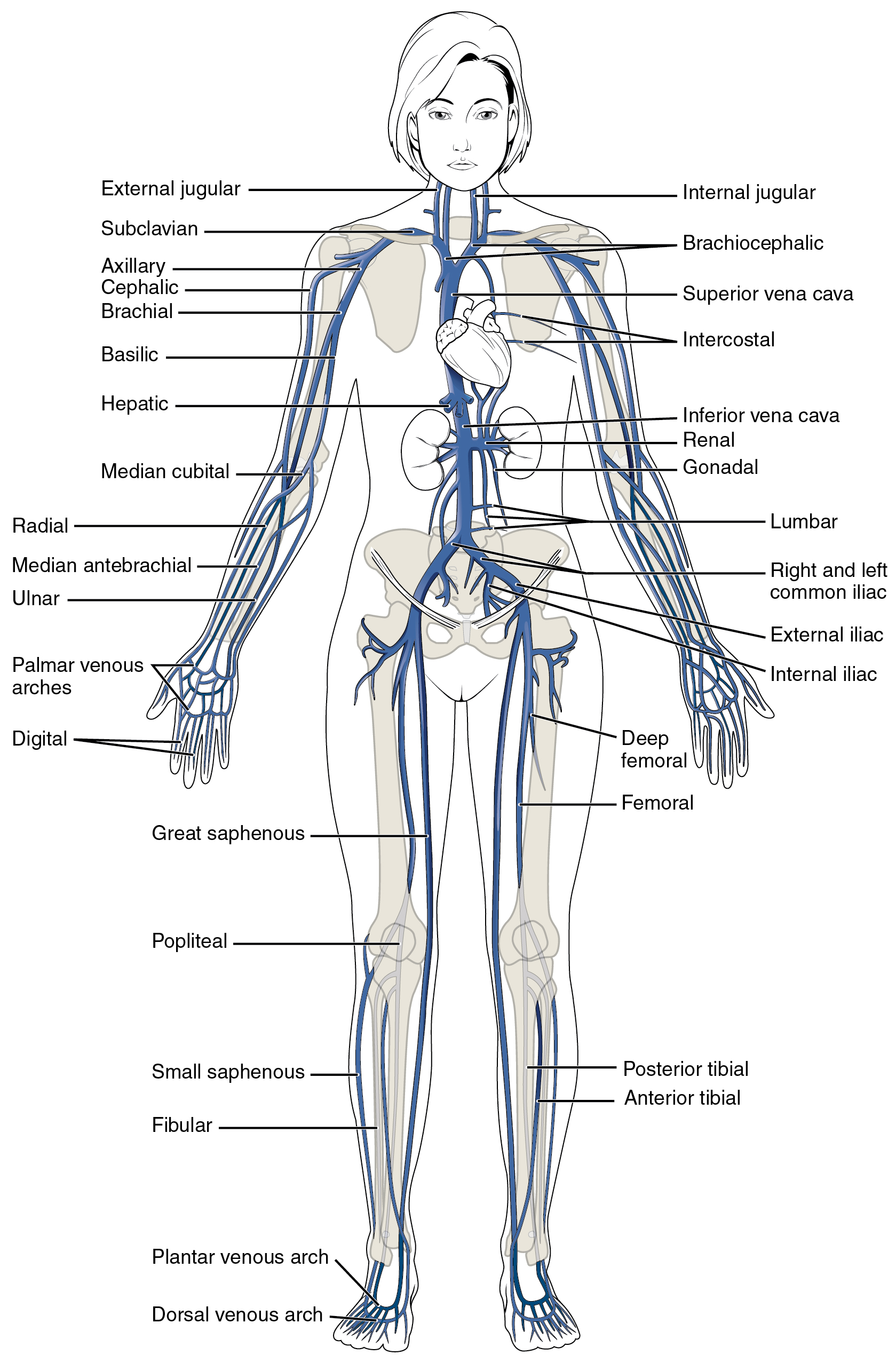
The Major Arteries and Veins in the Human Body
Concept Check
- Without looking back at the images of the main arteries and veins of the body, can you name and locate 3 arteries and 3 veins in your body?
Physiology of the Blood Vessels
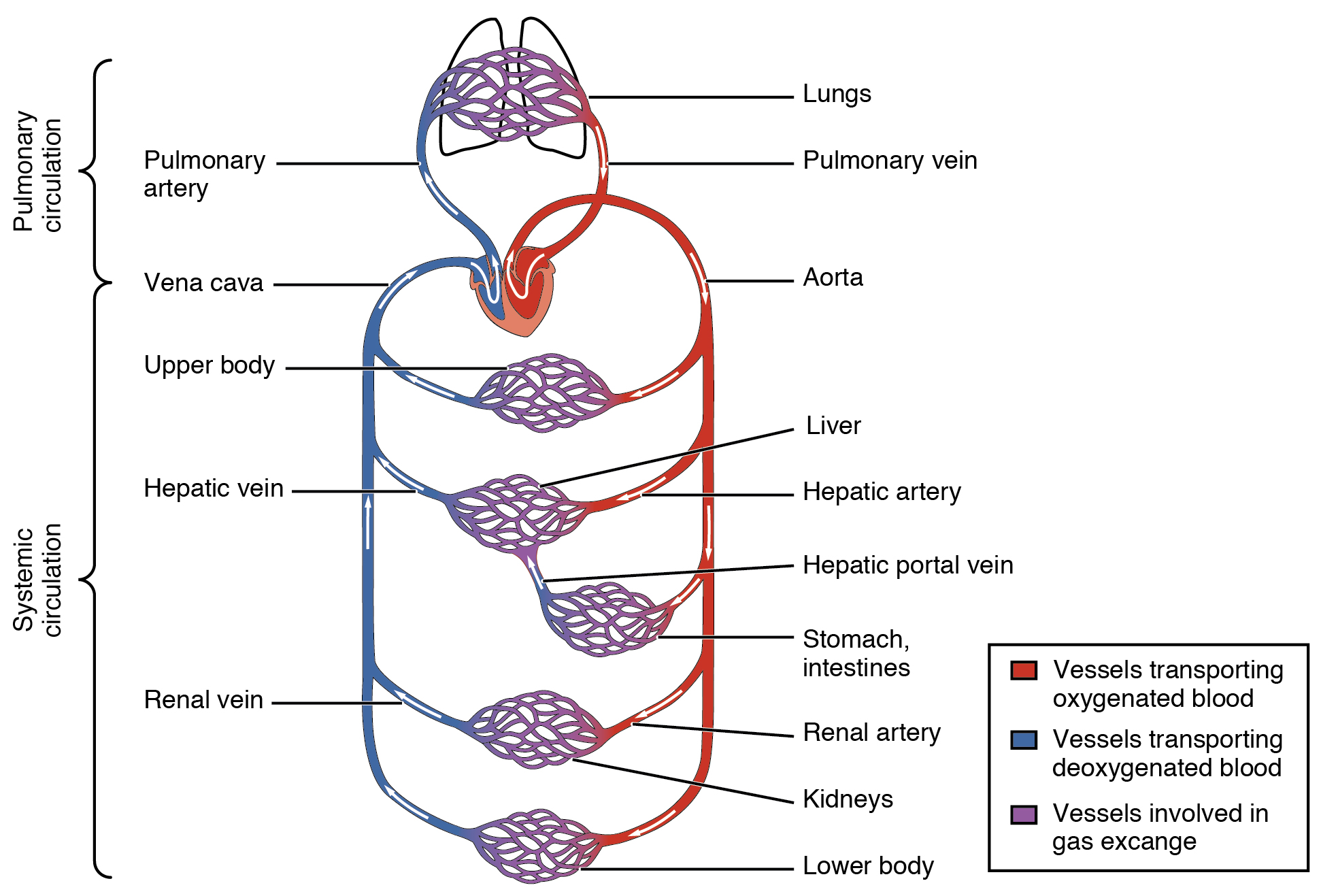
Arteries and veins transport blood in two distinct circuits: the systemic circuit and the pulmonary circuit. Systemic arteries provide blood rich in oxygen to the body’s tissues. The blood returned to the heart through systemic veins has less oxygen, since much of the oxygen carried by the arteries has been delivered to the cells. In contrast, in the pulmonary circuit, arteries carry blood low in oxygen exclusively to the lungs for gas exchange. Pulmonary veins then return freshly oxygenated blood from the lungs to the heart to be pumped back out into systemic circulation.
Blood Pressure
Five variables influence blood flow and blood pressure:
- Cardiac output
- Vessel Compliance
- Volume of the blood
- Viscosity of the blood
- Blood vessel length and diameter
Pulse
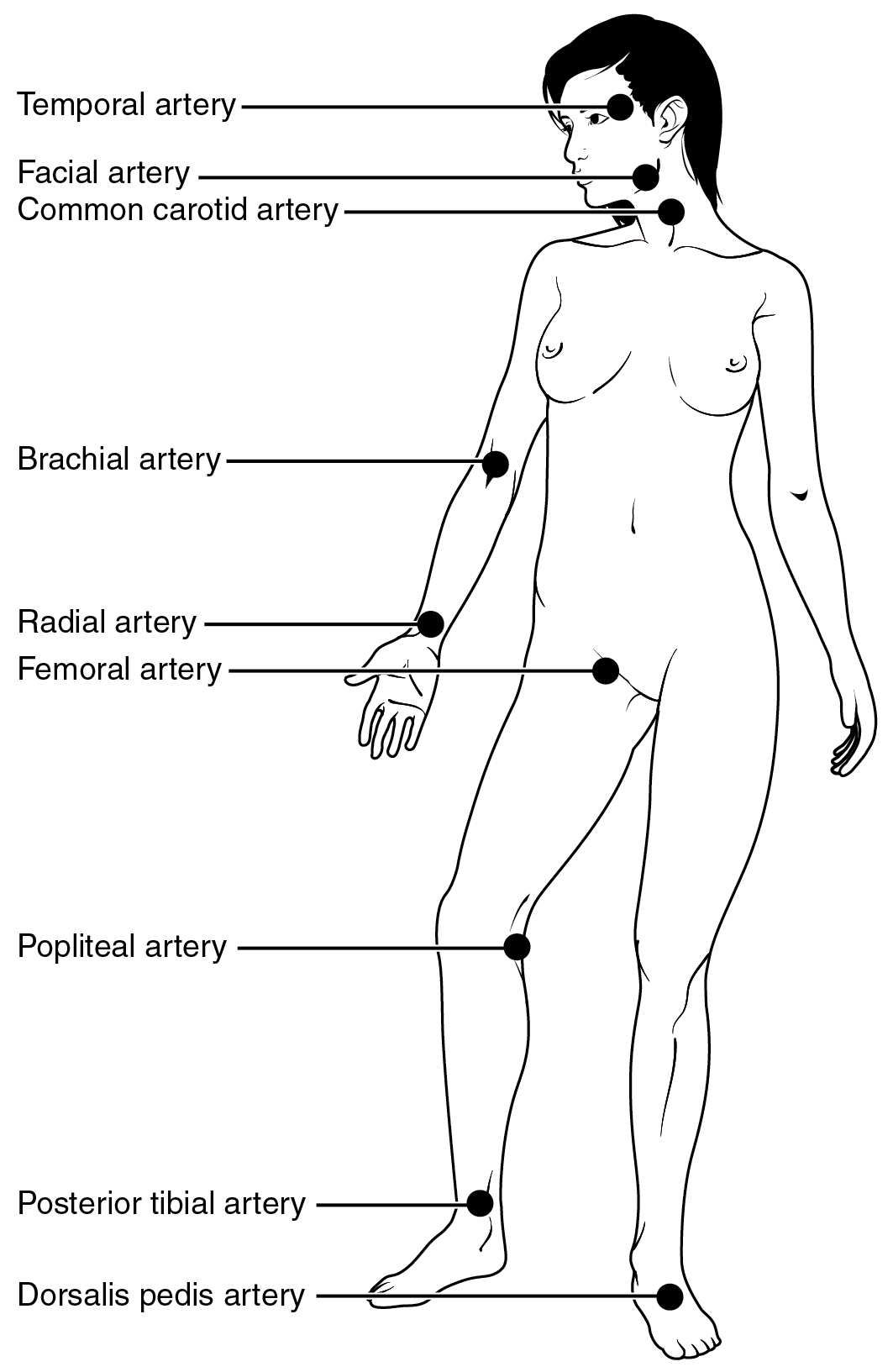
Each time the heart ejects blood forcefully into the circulation, the arteries must expand and then recoil to accommodate the surge of blood moving through them. This expansion and recoiling of the arterial wall is called the pulse and allows us to measure heart rate. Pulse can be palpated manually by placing the tips of the fingers across an artery that runs close to the body surface, such as the radial artery or the common carotid artery. These sites and other pulse sites are shown in the figure below.
Both the rate and the strength of the pulse are important clinically. A high or irregular pulse rate can be caused by physical activity or other temporary factors, but it may also indicate a heart condition. The pulse strength indicates the strength of ventricular contraction and cardiac output. If the pulse is strong, then systolic pressure is high. If it is weak, systolic pressure has fallen, and medical intervention may be warranted.
The Composition (Anatomy) of Blood and the Functions of the Components
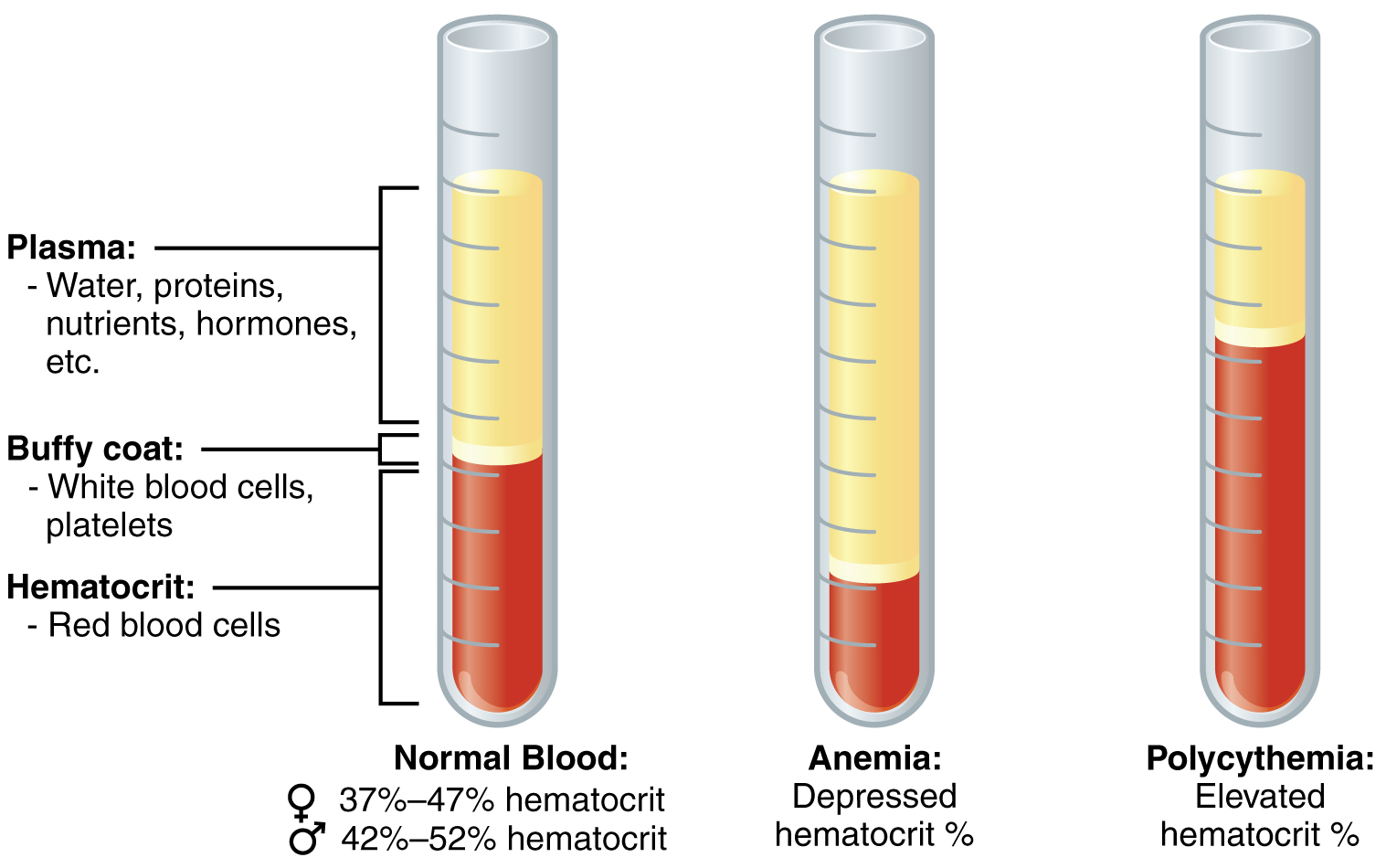
In the laboratory, blood samples are often centrifuged in order to separate the components of blood from one another (see the figure below). Erythrocytes are the heaviest elements in blood and settle at the very bottom of the tube. Above the erythrocyte layer we see the buffy coat, a pale, thin layer of leukocytes and thrombocytes, which together make up less than 1% of the sample of whole blood. Above the buffy coat is the blood plasma, normally a pale, straw-colored fluid, which constitutes the remainder of the sample.
In normal blood, about 45 percent of a sample is erythrocytes, which is referred to as the hematocrit. The hematocrit of any one sample can vary significantly, however, about 36–50 percent, according to gender and other factors. Not counting the buffy coat, which makes up less than 1% of the blood, we can estimate the mean plasma percentage to be the percent of blood that is not erythrocytes: approximately 55%.
| COMPONENT AND % OF BLOOD | SUBCOMPONENT AND % OF COMPONENT | TYPE AND % (WHERE APPROPRIATE) | SITE OF PRODUCTION | MAJOR FUNCTION(S) |
| Plasma 46 – 63 percent | Water 92 percent | Fluid | Absorbed by intestinal tract or produced by metabolism | Transport medium |
| Plasma proteins | Albumin 54 – 60 percent | Liver | Maintain osmotic concentration, transport lipid molecules | |
| Globulins 35 – 38 percent | Alpha globulins – liver | Transport, maintain osmotic concentration | ||
| Beta globulins – liver | Transport, maintain osmotic concentration | |||
| Gamma globulins (immunoglobulins) – plasma cells | Immune responses | |||
| Fibrinogen 4 – 7 percent | Liver | Blood clotting in hemostasis | ||
| Regulatory proteins < 1 percent | Hormones and enzymes | Various sources | Regulate various body functions | |
| Other solutes 1 percent | Nutrients, gases, and wastes | Absorbed by intestinal tract, exchanged in respiratory system, or produced by cells | Numerous and varied | |
| Formed elements 37 – 54 percent | Erythrocytes 99 percent | Erythrocytes | Red bone marrow | Transport gases, primarily oxygen and some carbon dioxide |
| Leukocytes < 1 percent Platelets < 1 percent |
Granular Leukocytes: neutrophils eosinophils basophils |
Red bone marrow | Nonspecific immunity | |
| Agranular leukocytes: lymphocytes monocytes |
Lymphocytes: bone marrow and lyphatic tissue |
Lymphocytes: specific immunity |
||
| Monocytes: redbone marrow | Monocytes: nonspecific immunity |
|||
| Platelets < 1 percent |
n/a | Megakaryocytes: Red Bone Marrow |
Hemostasis |
Concept Check
Use the table above to answer these questions:
- What substance makes up most of the plasma?
- What are some general functions of plasma and its components?
- What is the function of erythrocytes?
- What is the overall function of leukocytes? (Hint: which word appears in all 3 chart cells that list leukocyte functions?)
- What is the function of platelets?
Blood Plasma
Like other fluids in the body, plasma is composed primarily of water. In fact, it is about 92% water. Dissolved or suspended within this water is a mixture of substances, most of which are proteins. The major components of plasma and their functions are summarized in the table above.
Formed Elements (Erythrocytes, Leukocytes, Thrombocytes)
The table below summarizes the main facts about the formed elements in blood.
| FORMED ELEMENT | MAJOR SUBTYPES | NUMBER PRESENT PER MICROLITER (µL) AND MEAN (RANGE) | APPEARANCE IN A STANDARD BLOOD SMEAR | SUMMARY OF FUNCTIONS | COMMENTS |
|
Erythrocytes (red blood cells)  |
n/a | 5.2 million ( 4.4-5.0 million) | Flattened biconcave disk; no nucleus; pale red colour | Transport oxygen and some carbon dioxide between tissues and lungs | Lifespan of approximately 120 days |
| Leukocytes (white blood cells) | n/a | 7000 (5000 – 10,000) | Obvious dark-staining nucleus | All function in body defenses | Exit capillaries and move into tissues; lifespan of usually a few hours or days |
| Leukocytes (white blood cells) Types |
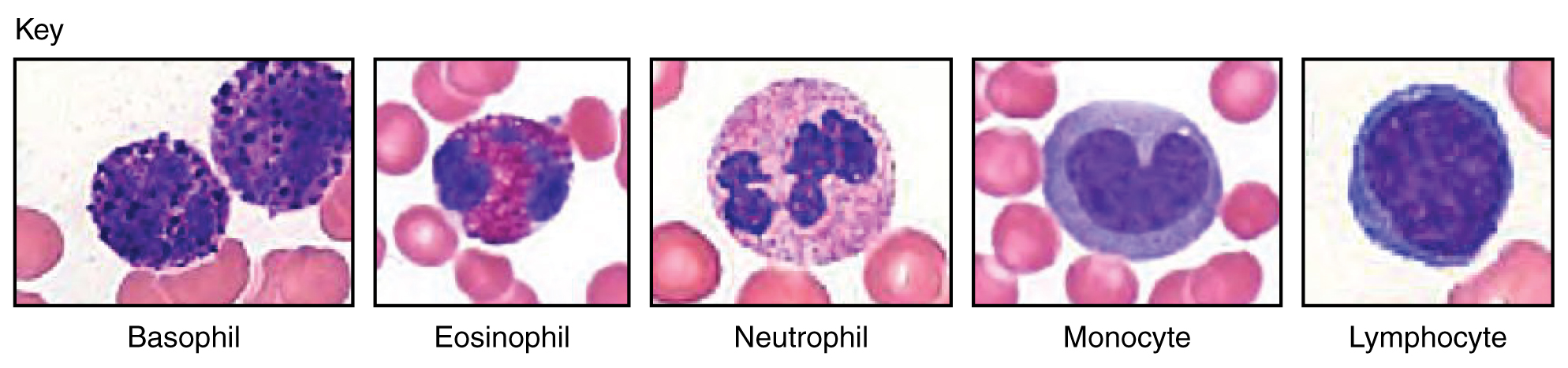
Granulocytes including neutrophils, eosinophils, and basophils | 4360 (1800-9950) | Abundant granules in cytoplasm; nucleus normal lobed | Nonspecific (innate) resistance to disease | Classified according to membrane-bound granules in cytoplasm |
|
Neutrophils  |
4150 (1800-7300) | Nuclear lobes increase with age; pale lilac granules | Phagocytic; particularly effective against bacteria. Release cytotoxic chemicals from granules | Most common leukocyte; lifespan of minutes to days | |
|
Eosinophils 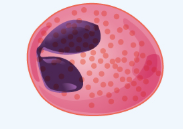 |
165 (0-700) | Nucleus generally two-lobed; bright red-orange granules | Phagocytic cells; particularly effective with antigen-antibody complexes. Release antihistamines. Increase in allergies and parasitic infections | Lifespan of minutes to days | |
|
Basophils 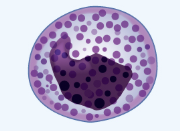 |
44 (0-150) | Nucleus generally two-lobed but difficult to see due to presence of heavy, dense, dark purple granules | Promotes inflammation | Least common leukocyte; lifespan unknown | |
| Agranulocytes including lymphocytes and monocytes | 2640 (1700-4950) | Lack abundant granules in cytoplasm; have a simple-shaped nucleus that may be indented | Body defenses | Group consists of two major cell types from different lineages | |
|
Lymphocytes  |
2185 (1500-4000) | Spherical cells with a single often large nucleus occupying much of the cell’s volume; stains purple; see in large (natural killer cells) and small (B and T cells) variants | Primarily specific (adaptive) immunity; T cells directly attack other cells (cellular immunity). B cells release antibodies (humoral immunity); natural killer cells are similar to T cells but nonspecific | Initial cells originate in bone marrow, but secondary production occurs in lymphatic tissue; several distinct subtypes; memory cells form after exposure to a pathogen and rapidly increase responses to subsequent exposure; lifespan of many years | |
|
Monocytes  |
455 (200-950) | Largest leukocyte with an indented or horseshoe-shaped nucleus | Very effective phagocytic cells engulfing pathogens or worn out cells; also serve as antigen-presenting cells (APCs) for other components of the immune system | Produced in red bone marrow; referred to as macrophages after leaving circulation | |
|
Platelets  |
n/a | 350,000 (150,000 – 500,000) | Cellular fragments surrounded by a plasma membrane and containing granules; purple stain | Hemostasis plus release growth factors for repair and healing of tissue | Formed from megakaryocytes that remain in the red bone marrow and shed platelets into circulation |
Hemopoiesis/Hematopoiesis
The lifespan of the formed elements is very brief. Although one type of leukocyte (memory cells) can survive for years, most erythrocytes, leukocytes, and platelets normally live only a few hours to a few weeks. Thus, the body must form new blood cells and platelets quickly and continuously, a process known as hemopoiesis.
In children, hemopoiesis can occur in the medullary cavity of long bones; in adults, the process is largely restricted to the cranial and pelvic bones, the vertebrae, the sternum, and the proximal epiphyses of the femur and humerus. Throughout adulthood, the liver and spleen maintain their ability to generate the formed elements. This process is referred to as extramedullary hemopoiesis. When a disease such as bone cancer destroys the bone marrow, causing hemopoiesis to fail, extramedullary hemopoiesis may be initiated .
Erythrocytes
The most abundant formed elements in blood, erythrocytes are basically sacs packed with an oxygen-carrying compound called hemoglobin. Production of erythrocytes in the red bone marrow occurs at the staggering rate of more than 2 million cells per second. For this production to occur, raw materials including iron, copper, zinc B-vitamins, glucose, lipids, and amino acids must be present in adequate amounts. Erythrocytes live only 120 days on average, and thus must be continually replaced. Worn-out erythrocytes are phagocytized by macrophages and their hemoglobin is broken down. The breakdown products are recycled or removed as wastes.

Leukocytes
Concept Check
- What is hemoglobin?
- Can you name the 5 types of leukocytes?
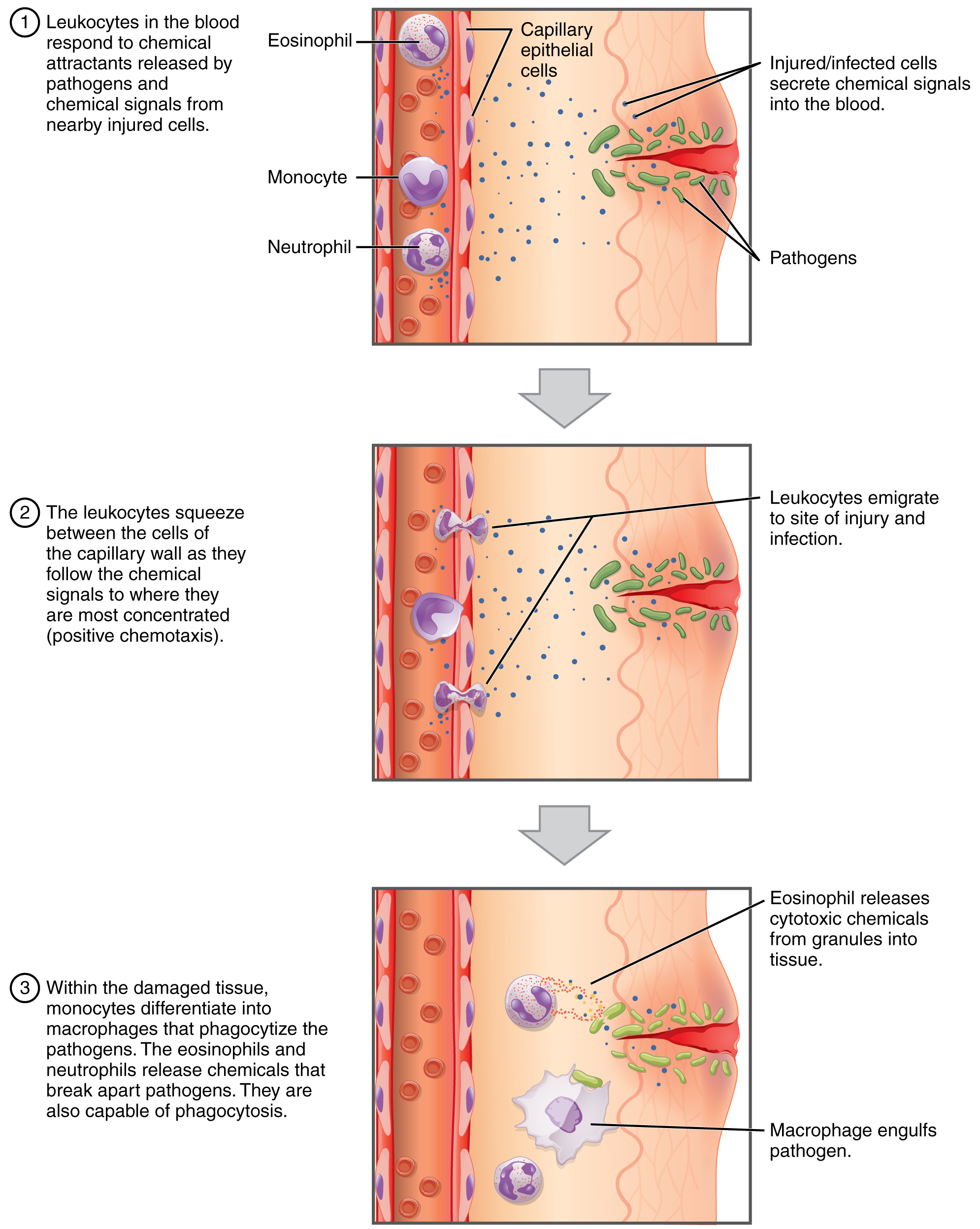
Leukocytes routinely leave the bloodstream to perform their defensive functions in the body’s tissues, where they are often given distinct names, such as macrophage or microglia, depending on their function. As shown in Figure 1 below, they leave the capillaries—the smallest blood vessels—or other small vessels through a process known as emigration or diapedesis in which they squeeze through adjacent cells in a blood vessel wall.
Once they have exited the capillaries, some leukocytes will take up fixed positions in lymphatic tissue, bone marrow, the spleen, the thymus, or other organs. Others will move about through the tissue spaces, sometimes wandering freely, and sometimes moving toward the direction in which they are drawn by chemical signals, a mechanism known as positive chemotaxis.
Lymphocytes
Lymphocytes are one of the types of leukocytes and will be discussed in more detail here, since they tie into the next chapter which discussed the body’s defenses The three major groups of lymphocytes include natural killer cells, B cells, and T cells.
-
- Natural killer (NK) cells are capable of recognizing cells that do not express “self” proteins on their plasma membrane or that contain foreign or abnormal markers. These “nonself” cells include cancer cells, cells infected with a virus, and other cells with atypical surface proteins.
- B lymphocytes (B cells) and T lymphocytes (T cells), play prominent roles in defending the body against specific pathogens (disease-causing microorganisms) and are involved in specific immunity. B cells undergo a maturation process in the bone marrow, whereas T cells undergo maturation in the thymus. This site of the maturation process gives rise to the name B and T cells.
- Plasma cells, a type of B cell, produce the antibodies or immunoglobulins that bind to specific foreign or abnormal components of plasma membranes.
- T cells provide immunity by physically attacking foreign or diseased cells.
- Memory cells are a variety of both B and T cells that form after exposure to a pathogen and mount rapid responses upon subsequent exposures. Unlike other leukocytes, memory cells live for many years.
Platelets
After entering the circulation, approximately one-third of the newly-formed platelets migrate to the spleen for storage for later release in response to any rupture in a blood vessel. They then become activated to perform their primary function, which is to limit blood loss. Platelets remain only about 10 days, then are phagocytized by macrophages.
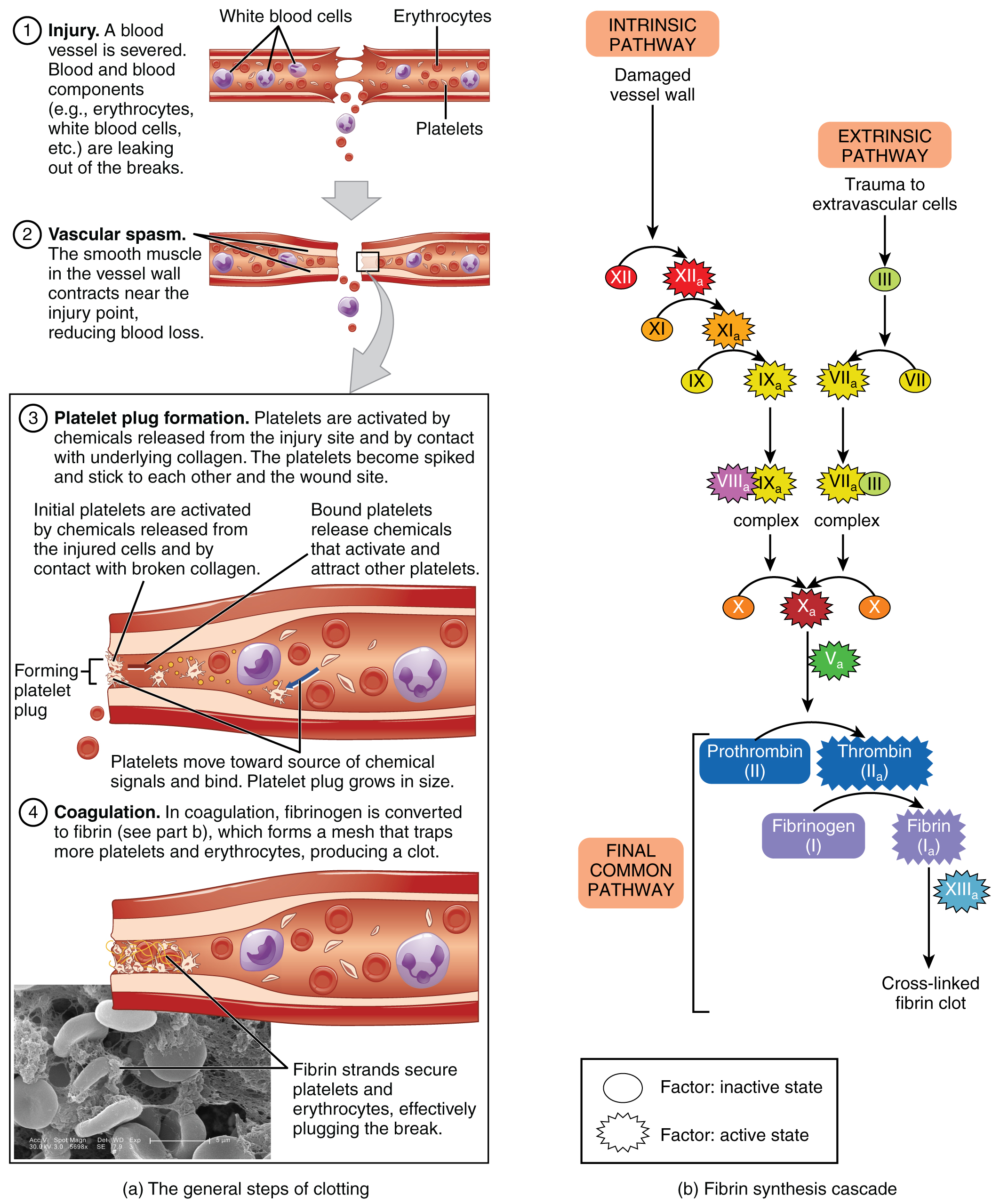
Platelets are key players in hemostasis, the process by which the body seals a ruptured blood vessel and prevents further loss of blood. Although rupture of larger vessels usually requires medical intervention, hemostasis is quite effective in dealing with small, simple wounds. There are three steps to the process: vascular spasm, the formation of a platelet plug, and coagulation (blood clotting). Failure of any of these steps will result in hemorrhage. The figure below summarizes the steps of hemostatis.
Fibrinolysis is the process in which a clot is degraded in a healing vessel. An anticoagulant is any substance that opposes coagulation. Several circulating plasma anticoagulants play a role in limiting the coagulation process to the region of injury and restoring a normal, clot-free condition of blood.
Concept Check
- Can you explain what happens in each step of hemostasis?
- Describe an anticoagulant.
Physiology of Blood
Although carrying oxygen and nutrients to cells and removing wastes from cells is the main function of blood, it is important to realize that blood also serves in defense, distribution of heat, and maintenance of homeostasis.
Transportation
- Nutrients from the foods you eat are absorbed in the digestive tract. Most of these travel in the bloodstream directly to the liver, where they are processed and released back into the bloodstream for delivery to body cells.
- Oxygen from the air you breathe diffuses into the blood, which moves from the lungs to the heart, which then pumps it out to the rest of the body.
- Endocrine glands scattered throughout the body release their products, called hormones, into the bloodstream, which carries them to distant target cells.
- Blood also picks up cellular wastes and byproducts, and transports them to various organs for removal. For instance, blood moves carbon dioxide to the lungs for exhalation from the body, and various waste products are transported to the kidneys and liver for excretion from the body in the form of urine or bile.
Defense
- Leukocytes protect the organism from disease-causing bacteria, cells with mutated DNA that could multiply to become cancerous, or body cells infected with viruses.
- When damage to the vessels results in bleeding, blood platelets and certain proteins dissolved in the plasma, interact to block the ruptured areas of the blood vessels involved. This protects the body from further blood loss.
Homeostasis
- If you were exercising on a warm day, your rising core body temperature would trigger several homeostatic mechanisms, including increased transport of blood from your core to your body periphery, which is typically cooler. As blood passes through the vessels of the skin, heat would be dissipated to the environment, and the blood returning to your body core would be cooler. In contrast, on a cold day, blood is diverted away from the skin to maintain a warmer body core. In extreme cases, this may result in frostbite.
- Blood helps to regulate the water content of body cells.
- Blood also helps to maintain the chemical balance of the body. Proteins and other compounds in blood act as buffers, which thereby help to regulate the pH of body tissues. The pH of blood ranges from 7.35 to 7.45.
Concept Check
These three terms all sound similar. Can you explain them by breaking down the word parts?
- Hemostasis
- Homeostasis
- Hemopoiesis
Blood Types
In order to understand blood types, it is important to understand several terms that relate to the body’s immune functions (discussed in detail in the next chapter)
- Antigens are substances that the body does not recognize as belonging to itself (“self”) and that therefore trigger a defensive response from the leukocytes of the immune system. Many people have antigens on the surfaces of their red blood cells. More than 50 antigens have been identified on erythrocyte membranes, but the most significant in terms of their potential harm to patients are classified in two groups: the ABO blood group and the Rh blood group.
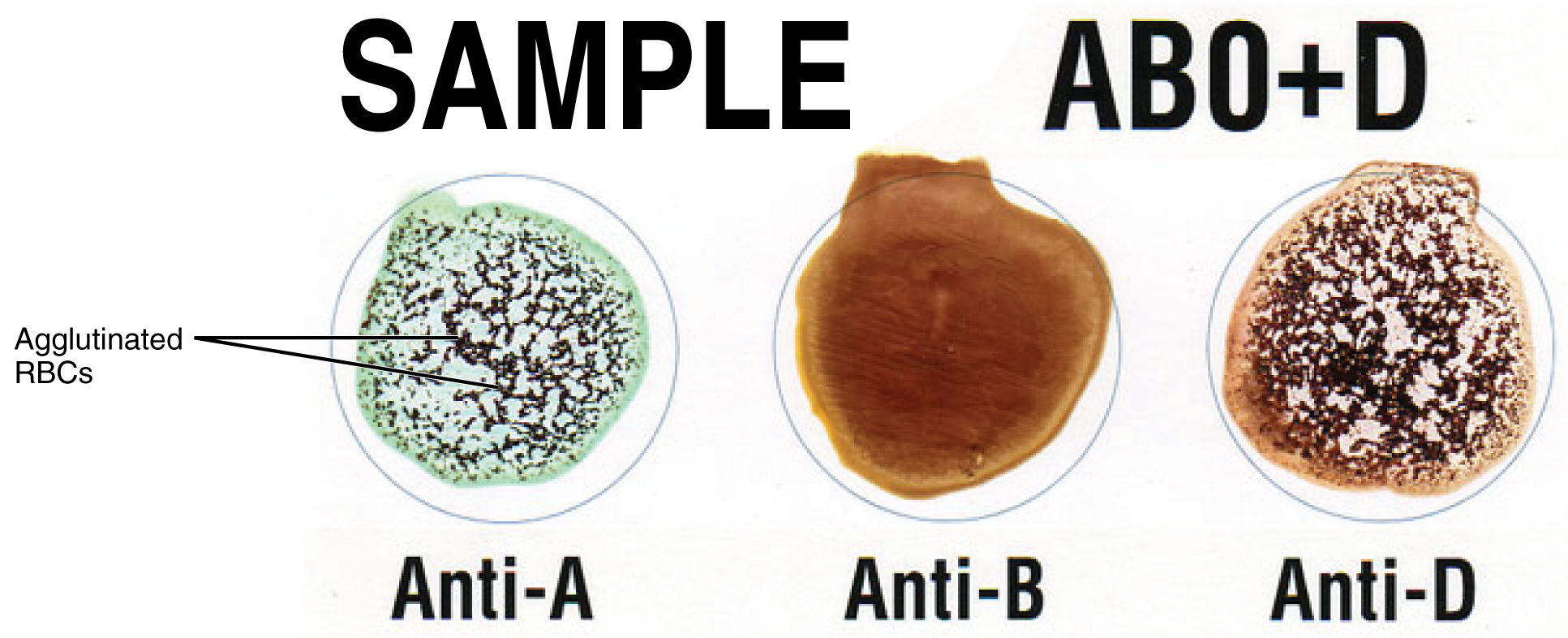
- Antibodies are proteins which are produced by plasma cells in response to a “non-self” antigen being present in the body. Antibodies attach to the antigens on the plasma membranes of the erythrocytes in a blood transfusion and cause them to adhere to one another.
- Agglutination refers to the resulting clumps of red blood cells that are formed in such an antigen-antibody reaction. These clumps can block small blood vessels, thereby cutting of the supply of oxygen and nutrients to the tissues.
- Hemolysis, or the breakdown of the erythrocyte’s cell membrane, takes place as the clumps of red cells start to degrade. The resulting release of the cell’s contents, mainly hemoglobin, into the bloodstream can cause kidney failure.
ABO Blood Group
ABO blood types are genetically determined. Each type is determined by the presence or absence of certain antigens on the individual’s red blood cell membrane, as well as the presence or absence of certain antibodies. Normally the body must be exposed to a foreign antigen before an antibody can be produced. This is not the case for the ABO blood group, in which some blood types come preloaded with their own set of antibodies against another type. The table below shows the ABO blood group as well as the universal donor and recipient in relation to blood transfusions.
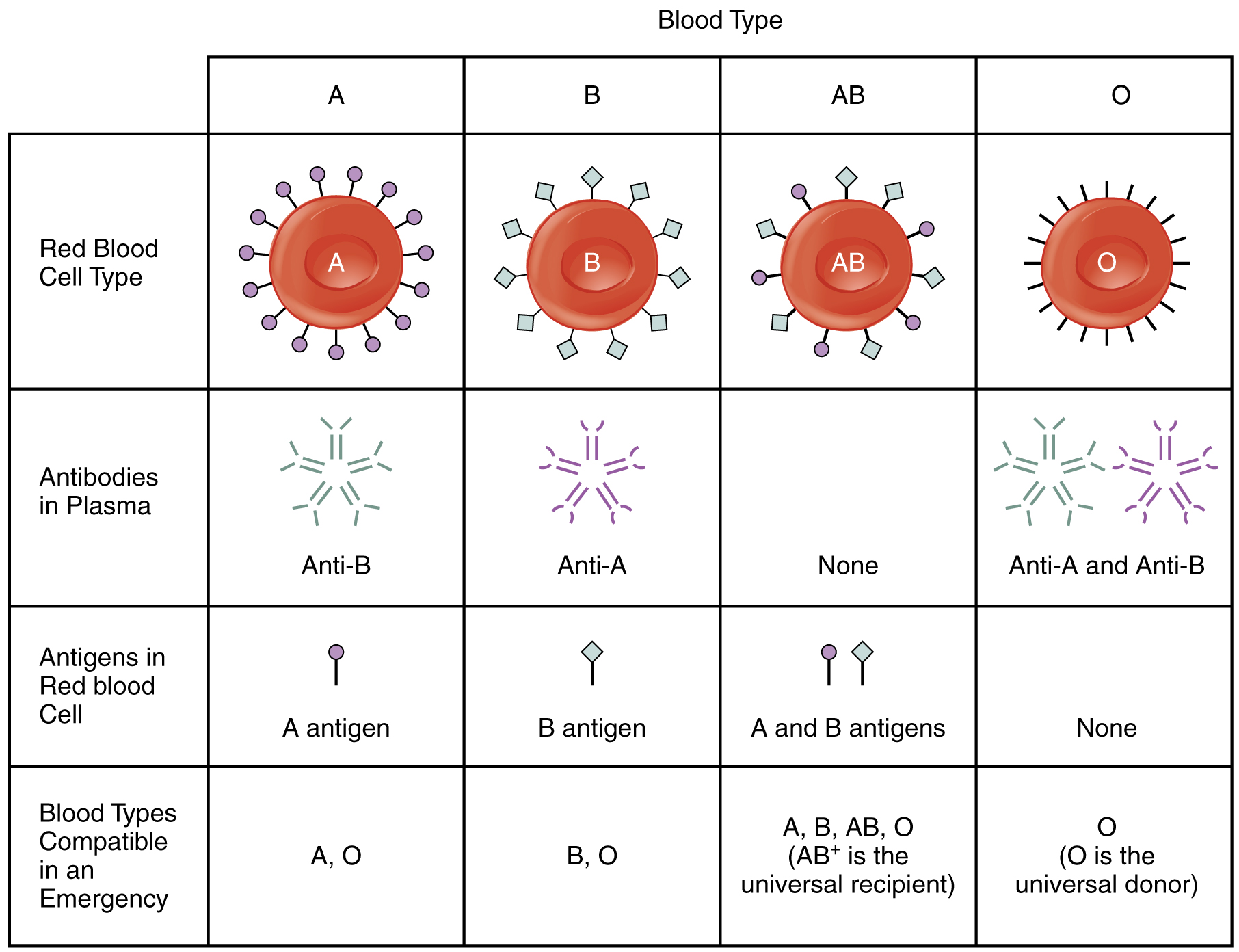
- Blood Type A
- People whose erythrocytes have A antigens on their erythrocyte membrane surface.
- People who have type A blood, without any prior exposure to incompatible blood, have preformed anti-B antibodies circulating in their blood. These antibodies will cause a serious immune reaction if they encounter blood that has B antigens.
- Blood Type B
- People whose erythrocytes have B antigens.
- People with type B blood has preformed anti-A antibodies.
- Blood Type AB
- People can also have both A and B antigens on their erythrocytes, in which case they are blood type AB.
- Individuals with type AB blood, do not have preformed antibodies to either A or B antigens.
- Blood Type O
- People with neither A nor B antigens are designated blood type O.
- People with type O blood have both anti-A and anti-B antibodies circulating in their blood plasma.
Rh Blood Group
The Rh blood group is classified according to the presence or absence of a second erythrocyte antigen identified as Rh. Those who have the Rh D antigen present on their erythrocytes are described as Rh positive (Rh+) and those who lack it are Rh negative (Rh−). Note that the Rh group is distinct from the ABO group, so any individual, no matter their ABO blood type, may have or lack this Rh antigen. When identifying a patient’s blood type, the Rh group is designated by adding the word positive or negative to the ABO type. For example, A positive (A+) means ABO group A blood with the Rh antigen present, and AB negative (AB−) means ABO group AB blood without the Rh antigen.
Hemolytic Disease of the Newborn (HDN)
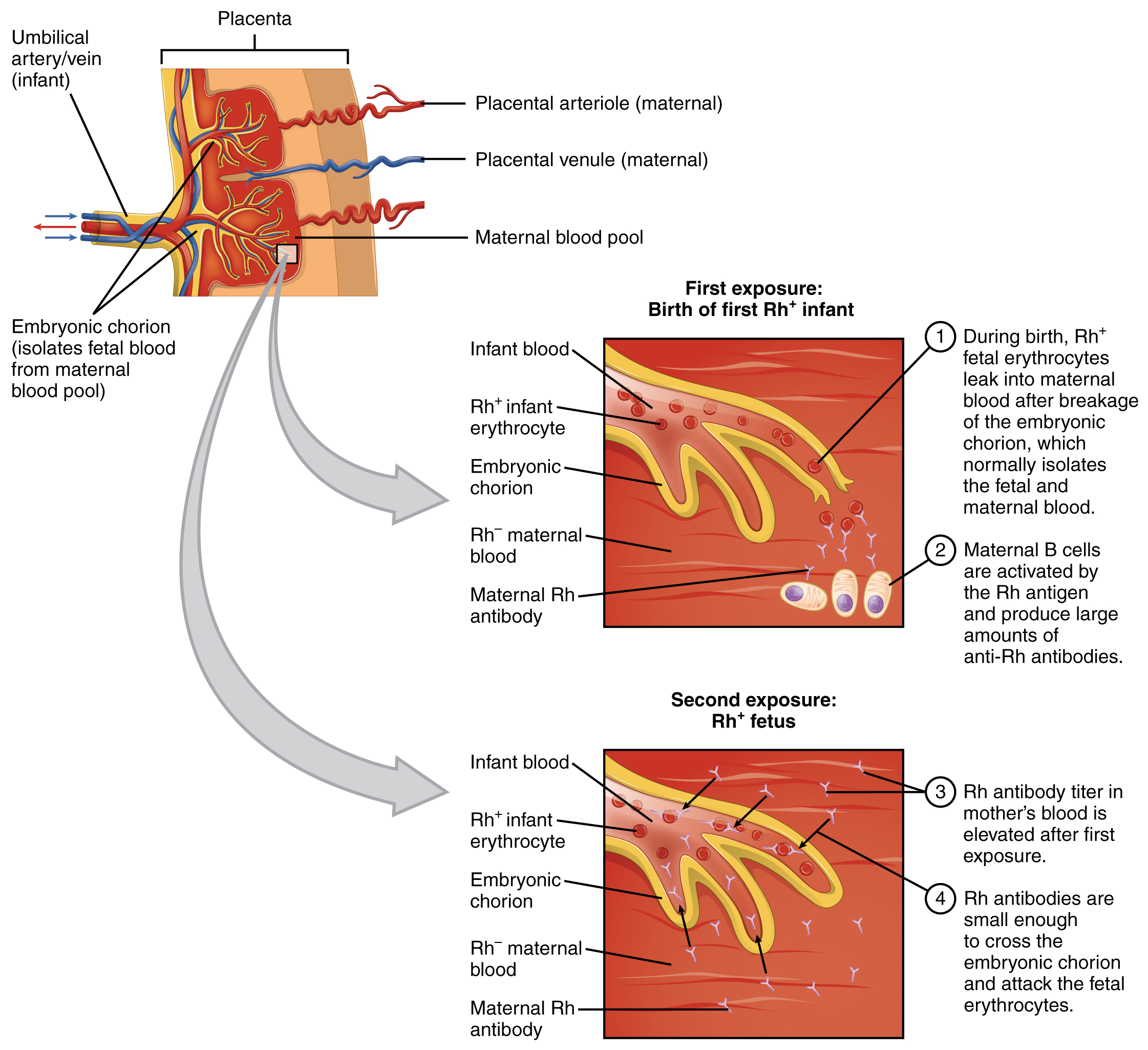
Antibodies to the Rh antigen are produced only in Rh− individuals after exposure to the antigen. This process, called sensitization, occurs following a transfusion with Rh-incompatible blood or, more commonly, with the birth of an Rh+ baby to an Rh− mother.
- In a first pregnancy problems are rare, since the baby’s Rh+ cells rarely cross the placenta. However, during or immediately after birth, the Rh− mother can be exposed to the baby’s Rh+ cells (Figure below). Research has shown that this occurs in about 13−14 percent of such pregnancies. After exposure, the mother’s immune system begins to generate anti-Rh antibodies.
- In a second pregnancy if a mother should conceive a Rh+ baby, the Rh antibodies she has produced can cross the placenta into the fetal bloodstream and destroy the fetal RBCs. This condition, known as hemolytic disease of the newborn (HDN) or erythroblastosis fetalis. This may cause anemia in mild cases, but the agglutination and hemolysis can be so severe that without treatment the fetus may die in the womb or shortly after birth.
- A drug known as RhoGAM, short for Rh immune globulin, can temporarily prevent the development of Rh antibodies in the Rh− mother, thereby averting this potentially serious disease for the fetus. RhoGAM antibodies destroy any fetal Rh+ erythrocytes that may cross the placental barrier. RhoGAM is normally administered to Rh− mothers during weeks 26−28 of pregnancy and within 72 hours following birth.
Blood Transfusions
To avoid transfusion reactions, it is best to transfuse only matching blood types; that is, a type B+ recipient should ideally receive blood only from a type B+ donor and so on. That said, in emergency situations, when acute hemorrhage threatens the patient’s life, there may not be time for cross matching to identify blood type. In these cases, blood from a universal donor may be transfused.
Blood Vessel Medical Terms Not Easily Broken into Word Parts
Common Diseases and Disorders of Blood Vessels and/or Blood
Arteriosclerosis
Arteriosclerosis is normally defined as the more generalized loss of compliance, “hardening of the arteries,” whereas atherosclerosis is a more specific term for the build-up of plaque in the walls of the vessel and is a specific type of arteriosclerosis.
When arteriosclerosis causes vessel compliance to be reduced, pressure and resistance within the vessel increase. This is a leading cause of hypertension and coronary heart disease, as it causes the heart to work harder to overcome this resistance. Any artery in the body can be affected by these pathological conditions, and individuals who have pathologies like coronary artery disease, may also be at risk for other vascular injuries, like strokes or peripheral arterial disease.
Atherosclerosis is a type of arteriosclerosis in which plaques form when circulating triglycerides, cholesterol and other substances seep between the damaged endothelial lining cells and become trapped within the artery wall, resulting in narrowed arteries and impaired blood flow (see Figure 13.16) (Betts, et al., 2013).
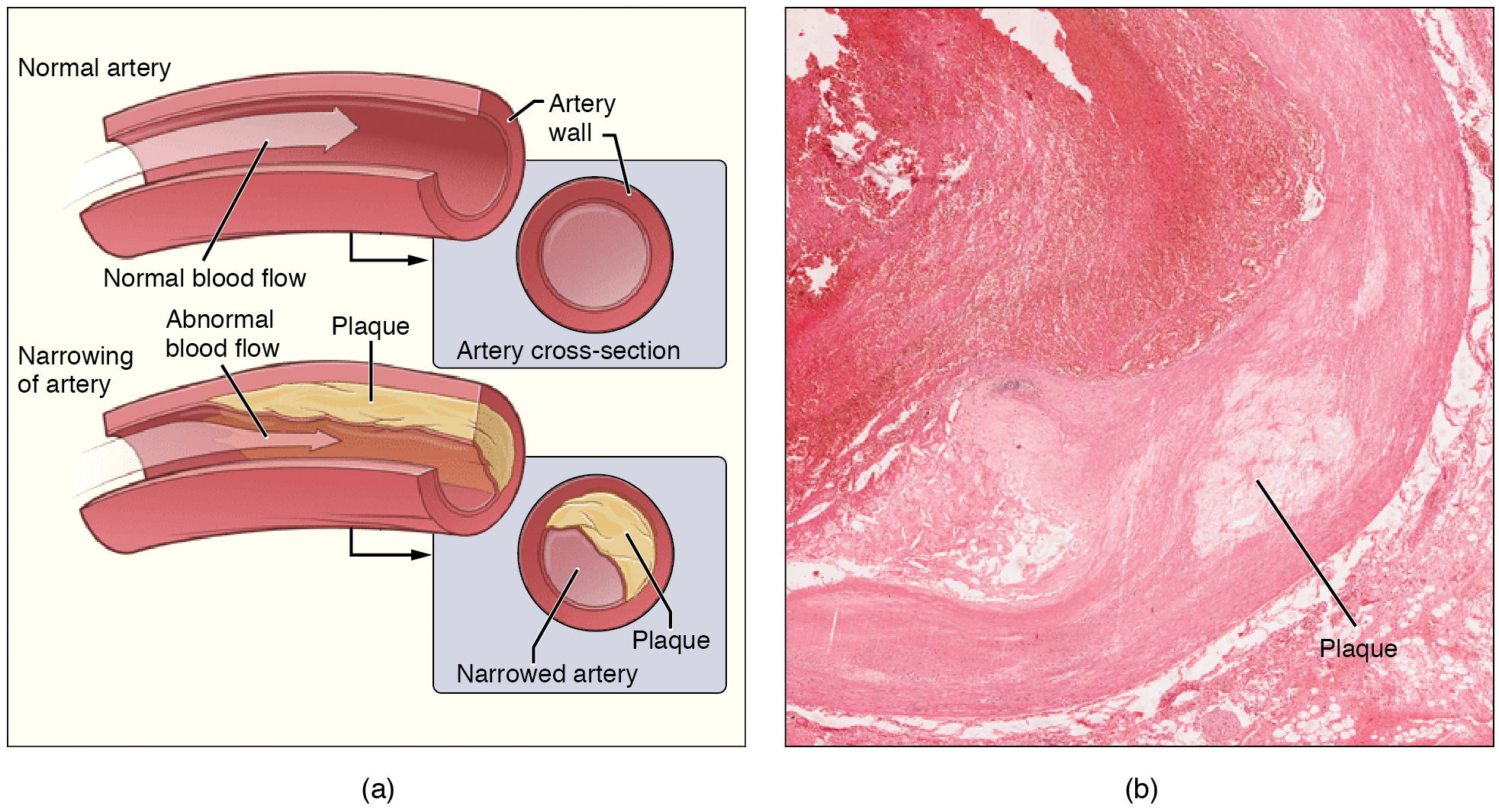
Sometimes a plaque can rupture, causing microscopic tears in the artery wall that allow blood to leak into the tissue on the other side. When this happens, platelets rush to the site to clot the blood. This clot can further obstruct the artery and—if it occurs in a coronary or cerebral artery—cause a sudden heart attack or stroke. Alternatively, plaque can break off and travel through the bloodstream as an embolus until it blocks a more distant, smaller artery.
Peripheral arterial disease (PAD, also called peripheral vascular disease, PVD), occurs when atherosclerosis affects arteries in the legs. A major risk factor for both arteriosclerosis and atherosclerosis is advanced age, as the conditions tend to progress over time. There is also a distinct genetic component, and pre-existing hypertension and/or diabetes also greatly increase the risk. However, obesity, poor nutrition, lack of physical activity, and tobacco use all are major risk factors.
Treatment of atherosclerosis includes lifestyle changes, such as weight loss, smoking cessation, regular exercise, and adoption of a diet low in sodium and saturated fats. Medications to reduce cholesterol and blood pressure may be prescribed. For blocked coronary arteries, angioplasty or coronary artery bypass graft (CABG) surgery may be warranted. In an carotid endarterectomy, plaque is surgically removed from the walls of a the carotid artery, which is the main source of oxygenated blood for the brain (Betts, et al., 2013).
Edema and Varicose Veins
Despite the presence of valves and the contributions of other anatomical and physiological adaptations that assist in moving blood through veins, over the course of a day, some blood will inevitably pool, especially in the lower limbs, due to the pull of gravity. Any blood that accumulates in a vein will increase the pressure within it, which can then be reflected back into the smaller veins, venules, and eventually even the capillaries. This increased pressure in the capillaries will push of fluids out of the capillaries and into the interstitial fluid, causing a condition called edema.
Most people experience a daily accumulation of tissue fluid, especially if they spend much of their work life on their feet (like most health professionals). However, clinical edema goes beyond normal swelling and requires medical treatment. Edema has many potential causes, including hypertension and heart failure, severe protein deficiency, renal failure, and many others. In order to treat edema, which is a sign rather than a discrete disorder, the underlying cause must be diagnosed and alleviated.

Edema may be accompanied by varicose veins, especially in the superficial veins of the legs (see Figure 13.17). This disorder arises when defective valves allow blood to accumulate within the veins, causing them to distend, twist, and become visible on the surface of the skin. Varicose veins may occur in both sexes, but are more common in women and are often related to pregnancy. More than simple cosmetic blemishes, varicose veins are often painful and sometimes itchy or throbbing. Without treatment, they tend to grow worse over time. The use of support hose, as well as elevating the feet and legs whenever possible, may be helpful in alleviating this condition (Betts, et al., 2013).
Hypertension
Hypertension is defined as chronic and persistent blood pressure measurements of 140/90 mm Hg or above. Pressures between 120/80 and 140/90 mm Hg are defined as prehypertension. Hypertension is typically a silent disorder and patients may fail to recognize the seriousness of their condition and fail to follow their treatment plan, putting them at risk for a heart attack or stroke. Hypertension may also lead to an aneurysm, peripheral arterial disease, chronic kidney disease, or heart failure (Betts, et al., 2013).
Hemorrhage
Minor blood loss is managed by hemostasis and repair. Hemorrhage is a loss of blood that cannot be controlled by hemostatic mechanisms. Initially, the body responds to hemorrhage by initiating mechanisms aimed at increasing blood pressure and maintaining blood flow. Ultimately, however, blood volume will need to be restored, either through physiological processes or through medical intervention. If blood loss is less than 20 percent of total blood volume, fast-acting homeostatic mechanisms causing increased cardiac output and vasoconstriction, would usually return blood pressure to normal and redirect the remaining blood to the tissues. Blood volume will then need to be restored via slower-acting homeostatic mechanisms, to increase body fluids and erythrocyte production (Betts, et al., 2013).
Circulatory Shock
The loss of too much blood may lead to circulatory shock, a life-threatening condition in which the circulatory system is unable to maintain blood flow to adequately supply sufficient oxygen and other nutrients to the tissues to maintain cellular metabolism. It should not be confused with emotional or psychological shock. Typically, the patient in circulatory shock will demonstrate an increased heart rate but decreased blood pressure. Urine output will fall dramatically, and the patient may appear confused or lose consciousness. Unfortunately, shock is an example of a positive-feedback loop that, if uncorrected, may lead to the death of the patient (Betts, et al., 2013).
There are several recognized forms of shock:
- Hypovolemic shock in adults is typically caused by hemorrhage, although in children it may be caused by fluid losses related to severe vomiting or diarrhea.
- Cardiogenic shock results from the inability of the heart to maintain cardiac output. Most often, it results from a myocardial infarction (heart attack), but it may also be caused by arrhythmias, valve disorders, cardiomyopathies, cardiac failure, or simply insufficient flow of blood through the cardiac vessels.
- Vascular shock occurs when arterioles lose their normal muscular tone and dilate dramatically. It may arise from a variety of causes, and treatments almost always involve fluid replacement and medications, called inotropic or pressor agents, which restore tone to the muscles of the vessels.
- Anaphylactic shock is a severe allergic response that causes the widespread release of histamines, triggering vasodilation throughout the body.
- Obstructive shock, as the name would suggest, occurs when a significant portion of the vascular system is blocked. It is not always recognized as a distinct condition and may be grouped with cardiogenic shock, including pulmonary embolism and cardiac tamponade. Treatments depend upon the underlying cause and, in addition to administering fluids intravenously, often include the administration of anticoagulants, removal of fluid from the pericardial cavity, or air from the thoracic cavity, and surgery as required. The most common cause is a pulmonary embolism. Other causes include stenosis of the aortic valve; cardiac tamponade; and a pneumothorax (Betts, et al., 2013).
Blood Disorders
Erythrocyte Disorders
Changes in the levels of RBCs can have significant effects on the body’s ability to effectively deliver oxygen to the tissues (Betts, et al., 2013).
Anemia
The size, shape, and number of erythrocytes, and the number of hemoglobin molecules can have a major impact on a person’s health. When the number of RBCs or hemoglobin is deficient, the general condition is called anemia. There are more than 400 types of anemia.
Anemia can be broken down into three major groups: those caused by blood loss, those caused by faulty or decreased RBC production, and those caused by excessive destruction of RBCs. In addition to these causes, various disease processes also can lead to anemias. These include chronic kidney diseases often associated with a decreased production of EPO, hypothyroidism, some forms of cancer, lupus, and rheumatoid arthritis(Betts, et al., 2013).
Blood Loss Anemias:
Causes:
- Bleeding from wounds or other lesions, including ulcers, hemorrhoids, inflammation of the stomach (gastritis), and some cancers of the gastrointestinal tract
- The excessive use of aspirin or other nonsteroidal anti-inflammatory drugs such as ibuprofen can trigger ulceration and gastritis
- Excessive menstruation and loss of blood during childbirth.
Anemias Caused by Faulty or Decreased RBC Production:
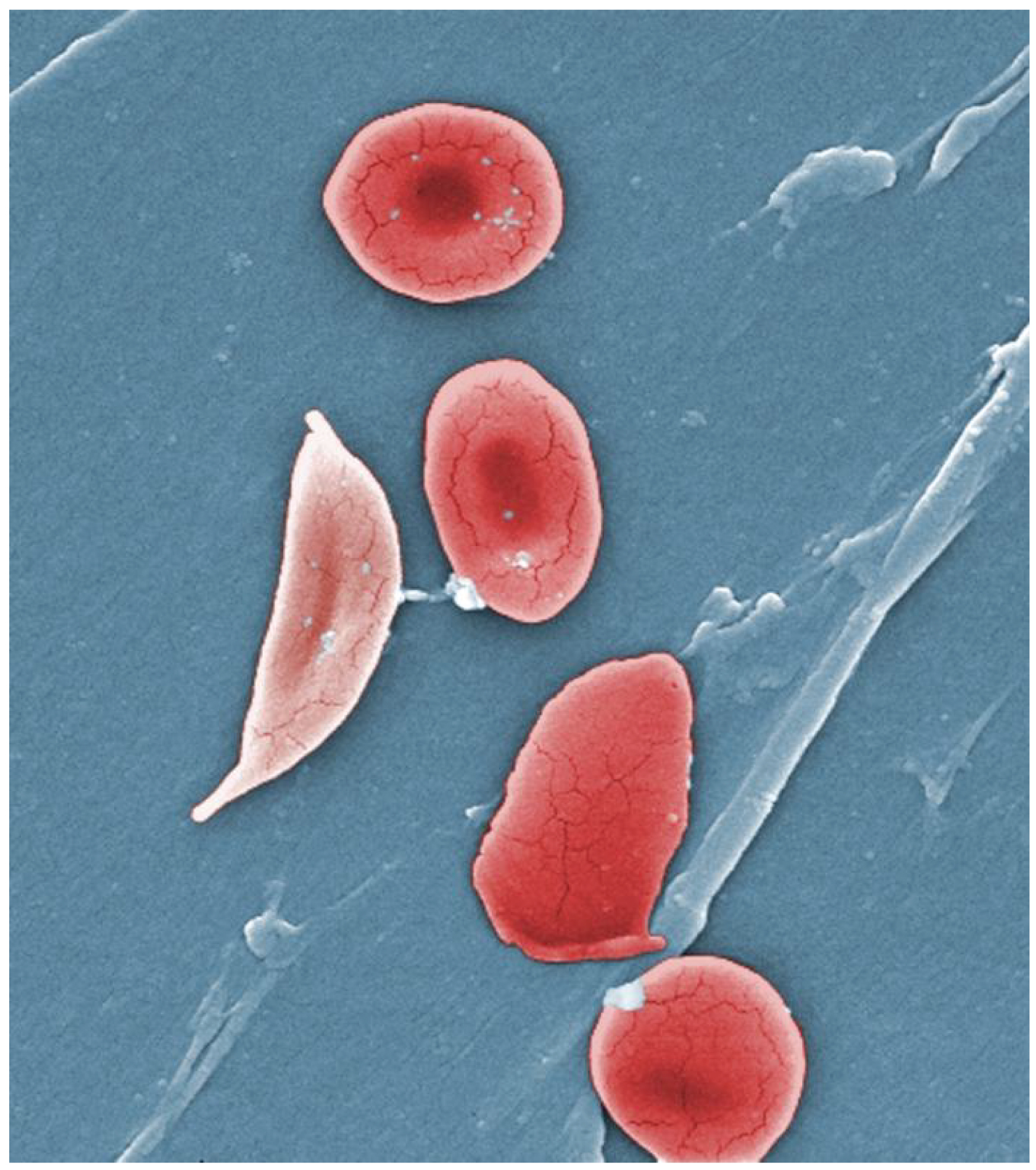
- Sickle cell anemia
-
- A genetic disorder involving the production of an abnormal type of hemoglobin which delivers less oxygen to tissues and causes erythrocytes to assume a sickle (or crescent) shape.
- Iron deficiency anemia
- The most common type of anemia and results when the amount of available iron is insufficient to allow production of sufficient heme.
- Vitamin deficiency anemia (Generally insufficient vitamin B12 and folate).
- Megaloblastic anemia involves a deficiency of vitamin B12 and/or folate, often due to inadequate dietary intake.
- Pernicious anemia is caused by poor absorption of vitamin B12 and is often seen in patients with Crohn disease, surgical removal of the intestines or stomach (common in some weight loss surgeries), intestinal parasites, and AIDS[/pb_glossary.
- Aplastic anemia is the condition in which myeloid stem cells are defective or replaced by cancer cells, resulting in insufficient quantities of RBCs being produced. This condition by be inherited, or it may be triggered by radiation, medication, chemotherapy, or infection.
- Thalassemia is an inherited condition typically occurring in individuals from the Middle East, the Mediterranean, African, and Southeast Asia, in which maturation of the RBCs does not proceed normally. The most severe form is called Cooley’s anemia (Betts, et al., 2013).
Polycythemia
Polycythemia is an elevated RBC count and is detected in a patient’s elevated [pb_glossary id="526"]hematocrit. It can occur transiently in a person who is dehydrated; when water intake is inadequate or water losses are excessive, the plasma volume falls. As a result, the hematocrit rises. A mild form of polycythemia is chronic but normal in people living at high altitudes. Some elite athletes train at high elevations specifically to induce this phenomenon. Finally, a type of bone marrow disease called polycythemia vera causes an excessive production of immature erythrocytes. Polycythemia vera can dangerously elevate the viscosity of blood, raising blood pressure and making it more difficult for the heart to pump blood throughout the body. It is a relatively rare disease that occurs more often in men than women, and is more likely to be present in elderly patients those over 60 years of age (Betts, et al., 2013).
Platelet Disorders/Clotting Disorders
Thrombocytosis
Thrombocytosis is a condition in which there are too many platelets. This may trigger thrombosis, a potentially fatal disorder. A thrombus (plural = thrombi) is an aggregation of platelets, erythrocytes, and even WBCs typically trapped within a mass of fibrin strands. While the formation of a clot is a normal step in hemostasis, thrombi can form within an intact or only slightly damaged blood vessel, adhering to the vessel wall and decreasing or obstructing the flow of blood. (Betts, et al., 2013).
Thrombophilia
Thrombophilia, also called hypercoagulation, is a condition in which there is a tendency to form thrombosis. This may be an inherited disorder or may be caused by other conditions including lupus, immune reactions to heparin, polycythemia vera, thrombocytosis, sickle cell disease, pregnancy, and even obesity.
When a portion of a thrombus breaks free from the vessel wall and enters the circulation, it is referred to as an embolus. An embolus that is carried through the bloodstream can be large enough to block a vessel critical to a major organ. When it becomes trapped, an embolus is called an embolism. In the heart, brain, or lungs, an embolism may accordingly cause a heart attack, a stroke, or a pulmonary embolism (Betts, et al., 2013).
Thrombocytopenia
Thrombocytopenia is a condition in which there is an insufficient number of platelets, possibly leading to ineffective blood clotting and excessive bleeding (Betts, et al., 2013).
Hemophilia
Hemophilia is a group of related genetic disorders in which certain plasma clotting factors are lacking or inadequate or nonfunctional. Patients with hemophilia bleed from even minor internal and external wounds, and leak blood into joint spaces after exercise and into urine and stool. Regular infusions of clotting factors isolated from healthy donors can help prevent bleeding in hemophiliac patients. At some point, genetic therapy will become a viable option (Betts, et al., 2013).
Leukocyte Disorders
Leukopenia
Leukopenia is a condition in which too few leukocytes are produced. If this condition is pronounced, the individual may be unable to ward off disease (Betts, et al., 2013).
Leukocytosis
Leukocytosis is excessive leukocyte proliferation. Although leukocyte counts are high, the cells themselves are often nonfunctional, leaving the individual at increased risk for disease (Betts, et al., 2013).
Leukemia
Leukemia is a cancer involving an abundance of leukocytes. It may involve only one specific type of leukocyte from either the myeloid line (myelocytic leukemia) or the lymphoid line (lymphocytic leukemia). In chronic leukemia, mature leukocytes accumulate and fail to die. In acute leukemia, there is an overproduction of young, immature leukocytes. In both conditions the cells do not function properly (Betts, et al., 2013).
Lymphoma
Lymphoma is a form of cancer in which masses of malignant T and/or B lymphocytes collect in lymph nodes, the spleen, the liver, and other tissues. As in leukemia, the malignant leukocytes do not function properly, and the patient is vulnerable to infection. Some forms of lymphoma tend to progress slowly and respond well to treatment. Others tend to progress quickly and require aggressive treatment, without which they are rapidly fatal (Betts, et al., 2013).
Other Conditions Related to Abnormal Leukocyte Counts
| CELL TYPE | CONDITIONS RELATED TO HIGH COUNTS | CONDITIONS RELATED TO LOW COUNTS |
| Neutrophil | Infection, inflammation, burns, unusual stress | Drug toxicity, other disorders |
| Eosinophil | Allergies, parasitic worm infestations, some autoimmune diseases | Drug toxicity, stress |
| Basophil | Allergies, parasitic infections, hypothyroidism | Pregnancy, stress, hyperthyroidism |
| Lymphocyte | Viral infections, some cancers | chronic illness, immunosuppression (due to HIV or steroid therapy) |
| Monocyte | Viral or fungal infections, tuberculosis, some forms of leukemia, other chronic diseases | Bone marrow suppression |
Bone Marrow Biopsy/Bone Marrow Transplant
Sometimes, a healthcare provider will order a bone marrow biopsy, a diagnostic test of a sample of red bone marrow, or a bone marrow transplant, a treatment in which a donor’s healthy bone marrow—and its stem cells—replaces the faulty bone marrow of a patient. These tests and procedures are often used to assist in the diagnosis and treatment of various severe forms of anemia, such as thalassemia major and sickle cell anemia, as well as some types of cancer, specifically leukemia.
In the past, bone marrow sampling or transplant was very painful, as the procedure involved inserting a large-bore needle into the region near the iliac crest of the pelvic bones. Now, direct sampling of bone marrow can often be avoided as stem cells can be isolated in just a few hours from a sample of a patient’s blood. The isolated stem cells are then grown in culture using the appropriate hemopoietic growth factors, and analyzed or sometimes frozen for later use.
For an individual requiring a transplant, a matching donor is essential to prevent the immune system from destroying the donor cells—a phenomenon known as tissue rejection. To treat patients with bone marrow transplants, it is first necessary to destroy the patient’s own diseased marrow through radiation and/or chemotherapy. Donor bone marrow stem cells are then infused into the recipient's bloodstream, so that they can establish themselves in the recipient’s bone marrow (Betts, et al., 2013).
Common Cardiovascular System - Blood, Abbreviations
Many terms and phrases related to the cardiovascular system - blood are abbreviated. Learn these common abbreviations by expanding the list below.
Medical Terms in Context
Medical Specialties and Procedures Related to the Blood Vessels and Blood
Vascular Surgeons
Vascular surgery is a specialty in which the physician treats diseases of the blood and lymphatic vessels. This includes repair and replacement of diseased or damaged vessels, removal of plaque from vessels, minimally invasive procedures including the insertion of venous catheters, and traditional surgery (Betts, et al., 2013; Canadian Society for Vascular Surgery, n.d.). For more information, please visit Canadian Society for Vascular Surgery website.
Hematologists
Hematologists are specialist physicians that diagnose and treat blood disorders. These physicians must be well-versed in a wide array of laboratory procedures, basic medical disciplines, and clinical medicine (Canadian Medical Association, 2018). To learn more about hematologists, visit the Canadian Medical Association's specialty profile on hematology (PDF file).
Diagnostic Vascular Technologist
Also known as Canadian Registered Vascular Sonographers (CRVS®), these specialists are technologists that image the vascular system (Sonography Canada, 2020). To learn more, visit the Sonography Canada Credentials web page.
Phlebotomist
Phlebotomists are professionals trained to draw blood (phleb- = “a blood vessel”; -tomy = “to cut”). When more than a few drops of blood are required, phlebotomists perform a venipuncture, typically of a surface vein in the arm. They perform a capillary stick on a finger, an earlobe, or the heel of an infant when only a small quantity of blood is required. An arterial stick is collected from an artery and used to analyze blood gases. After collection, the blood may be analyzed by medical laboratories or perhaps used for transfusions, donations, or research (Betts, et al., 2013).
Medical Laboratory Technologist/Assistant
Medical or clinical laboratories employ a variety of individuals in technical positions. Training is provided through a variety of institutions and certification is through the Canadian Society for Medical Laboratory Science. Two specialized positions are:
- Medical laboratory technologists (MLT) perform complex analyses of tissue, blood and other body fluids.
- Medical laboratory assistants (MLA) spend the majority of their time processing samples, and in some cases, collecting them (Canadian Society for Medical Laboratory Science, n.d.)
Cardiovascular System-Blood Vocabulary
ABG
Arterial blood gas. This test measures blood pH, oxygen and CO2 levels in a sample of arterial blood, usually taken from the wrist.
AIDS
Acquired immunodeficiency syndrome, caused by infection with the HIV virus.
Aneurysm
Weakening of the wall of a blood vessel, causing it to thin and balloon out, and possibly eventually burst, resulting in internal bleeding.
Angioplasty
A balloon-tip catheter is fed through a blood vessel up to the site of the narrowing, the balloon is inflated to re-open the artery. A stent is sometimes placed at the site to reinforce the arterial wall and to prevent re-occlusion.
Anti-B Antibodies
Proteins that will mount an immune response against B antigens.
Antibodies
Also called immunoglobulins, proteins produced by B lymphocytes in response to a non-self antigen.
Antigens
A substance that provokes an immune response. This happens because the immune system sees the antigen as foreign, or 'non-self" (does not belong in that body).
Arteries
Blood vessels that transport blood away from the heart.
Arterioles
A very small artery that leads to a capillary.
Arteriosclerosis
Hardening of arteries.
Atherosclerosis
A hardening of the arteries that involves the accumulation of plaque.
Brachial Artery
Large artery in the upper arm near the biceps muscle.
Capillary
A microscopic channel that supplies blood to the tissues through perfusion.
Cardiac Output
Cardiac output is the measurement of blood flow from the heart through the ventricles, and is usually measured in liters per minute. Any factor that causes cardiac output to increase, by elevating heart rate or stroke volume or both, will elevate blood pressure and promote blood flow.
Cardiac Tamponade
The pericardial sac surrounding the heart has filled with blood or other fluid and the resulting pressure is preventing the heart from beating effectively.
Cardiogenic
Originating from the heart.
Carotid Artery
A large artery in the neck.
Celiac Disease
Inflammation of the intestines caused by exposure to gluten.
Centrifuged
A centrifuge is a common piece of laboratory equipment used to spin test tubes at a high speed in order to separate components in a liquid by weight.
Chemoreceptors
Cells that sense changes in chemical levels.
Chemotaxis
Movement in response to chemicals; a phenomenon in which injured or infected cells and nearby leukocytes emit the equivalent of a chemical “911” call, attracting more leukocytes to the site.
Compliance
The ability of any compartment to expand to accommodate increased content. The greater the compliance of an artery, the more effectively it is able to expand to accommodate surges in blood flow without increased resistance or blood pressure.
Coronary Artery Bypass Graft (CABG)
In a coronary bypass procedure, a non-vital superficial vessel from another part of the body (often the great saphenous vein) or a synthetic vessel is inserted to create a path around the blocked area of a coronary artery.
Coronary Heart Disease
Also called coronary artery disease (CAD); the blood vessels that supply blood to the myocardium become hardened and narrowed, impairing the delivery of oxygen to the heart muscle.
Crohn Disease
A type of inflammatory bowel disease.
Diapedesis
dia- = “through”; -pedan = “to leap”
Diastolic Pressure
The diastolic pressure is the lower value (usually about 80 mm Hg) and represents the arterial pressure of blood during ventricular relaxation, or diastole.
Edema
Swelling.
Embolus
A freely moving piece of a substance (plaque or blood clot) that travels through the circulation until it blocks a smaller blood vessel, cutting of the supply of oxygen to the tissue.
Endothelium
The lining of the lumen of a blood vessel.
Epiphyses
The ends of long bones, singular is epiphysis.
EPO
Erythropoietin is a hormone produced by the kidneys that plays an important role in the homeostasis of red blood cells levels in the body.
Erythrocytes
Red blood cells.
Extramedullary Hemopoiesis
Hemopoiesis outside the medullary cavity of adult bones.
Heart Rate
The number of times the heart contracts in one minute.
Hematocrit
A lab test which measures the percentage red blood cells in a sample of whole blood. It represents how much of the person's blood is made up of red blood cells, by volume.
Hemolysis
Breaking apart of the erythrocyte cell membrane, allowing its contents to leak out.
Hemopoiesis
Also called hematopoiesis; from the Greek root haima- = “blood”; -poiesis = “production”.
Hemopoietic Growth Factors
Chemical messengers which promote the proliferation and differentiation of formed elements and include erythropoietin, thrombopoietin, colony-stimulating factors, and interleukins.
Hemorrhage
Excessive or uncontrolled bleeding from the blood vessels.
Hemostasis
The process by which the body seals a ruptured blood vessel to prevent further blood loss.
Homeostasis
Biological process that results in stable equilibrium.
Hypertension
High blood pressure.
Hypothyroidism
Underactive thyroid gland, insufficient production of thyroid hormones (T3 and T4).
Hypovolemic
hypo=below, lower than normal, volemic=pertaining to volume (in this case, the volume of blood in the body).
Hypoxemia
Low blood oxygen levels.
Hypoxia
Literally: 'lower than normal amount of oxygen to tissues'. Hypoxia means that a tissue is not getting enough oxygen to survive and cell death is likely.
Ischemia
Insufficient blood and oxygen to cells of an organ. These cells are starving for oxygen, but they are still alive.
Leukocytes
White blood cells.
Lupus
An autoimmune disease in which the body mounts an immune response against its own tissues, causing chronic inflammation and tissue damage.
Macrophages
A type of leukocyte (usually a monocyte) that has the ability to ingest and destroy other cells or pathogens.
Medulla Oblongata
A part of the brain stem responsible for control of heart rate and breathing.
Perfusion
The delivery of blood to an area/tissue/organ.
Peripheral Arterial Disease
The obstruction of vessels in peripheral regions of the body.
pH
A measure of how acidic or alkaline a substance is, as determined by the number of free hydrogen ions in the substance.
Phagocytized
Also phagocytosed, this is the process by which certain cells are able to 'eat' other cells or substances by engulfing them
Placenta
The organ of gas and nutrient exchange between the baby and the mother.
Plaque
A fatty material including cholesterol, connective tissue, white blood cells, and some smooth muscle cells.
Plasma Cells
A type of B lymphocyte that produces antibodies which bind to specific foreign or abnormal antigens, in order to destroy them.
Pneumothorax
An excessive amount of air is present in the thoracic cavity, outside of the lungs, putting pressure on the lungs and interfering with venous return, pulmonary function, and delivery of oxygen to the tissues.
Polycythemia Vera
A type of bone marrow disease that causes an excessive production of immature erythrocytes.
Pulmonary Embolism
A piece of a blood clot or other substance has broken free from its original location and traveled through the bloodstream to lodge in a smaller vessel in the lungs. This causes an obstruction in that vessel and hypoxia to the tissues supplied by that vessel.
Rheumatoid Arthritis
An autoimmune disorder in which the body mounts an immune response against its own joint tissues, causing inflammation and damage to the joints.
Sickle Cell Disease
Also called sickle cell anemia: A genetic disorder involving the production of an abnormal type of hemoglobin which delivers less oxygen to tissues and causes erythrocytes to assume a sickle (or crescent) shape.
Silent Disorder
A disease or disorder that often lacks signs or symptoms.
Sphygmomanometer
A blood pressure cuff attached to a measuring device, or gauge.
Systolic Pressure
The systolic pressure is the higher value (typically around 120 mm Hg) and reflects the arterial pressure resulting from the ejection of blood during ventricular contraction, or systole.
Thalassemia
An inherited condition typically occurring in individuals from the Middle East, the Mediterranean, African, and Southeast Asia, in which maturation of the RBCs does not proceed normally. The most severe form is called Cooley’s anemia.
Thrombocytes
Also called platelets, these are cell fragments that aid in blood clotting.
Thrombocytosis
A condition in which there are too many platelets.
Thrombosis
Formation of unwanted blood clots.
Tissue Rejection
Also called organ rejection. The recipient's immune system recognizes the transplanted tissue, the graft, as non-self and mounts an immune response against it, ultimately destroying it.
Vasoconstrict
The smooth muscle layer in the blood vessel wall contracts, causing the vessel diameter to narrow. This increases blood pressure in the vessel.
Vasodilate
The smooth muscle layer in the wall of the blood vessel relaxes, allowing the vessel to widen. This decreases blood pressure in the vessel.
Vein
Blood vessels that carry blood back to the heart.
Venules
Extremely small veins.
Vessel Compliance
The ability of any compartment to expand to accommodate increased content. The greater the compliance of an artery, the more effectively it is able to expand to accommodate surges in blood flow without increased resistance or blood pressure.
Viscosity
The thickness of fluids that affects their ability to flow.
Test Yourself
References
Canadian Medical Association. (2018, August). Hematology profile. CMA Specialty Profiles. https://www.cma.ca/sites/default/files/2019-01/hematology-e.pdf
Canadian Society for Medical Laboratory Science. (n.d.). Who are lab professionals. https://www.csmls.org/Medical-Laboratory-Professionals/About/Who-are-Lab-Professionals.aspx
Canadian Society for Vascular Surgery. (2020). Patients: What is vascular surgery? https://canadianvascular.ca/Patients
[CrashCourse]. (2015, July 20). Blood vessels, part 1 - form and function: Crash course A&P #27 [Video]. YouTube. https://youtu.be/v43ej5lCeBo
Sonography Canada. (2020). Credentials. https://sonographycanada.ca/certification/credentials
Image Descriptions
Figure 13.1 image description: The left panel shows the structure of a skeletal muscle vein pump when the muscle is relaxed, and the right panel shows the structure of a skeletal muscle vein pump when the muscle is contracted.[Return to Figure 13.1].
Figure 13.2 image description: The top left panel of this figure shows the ultrastructure of an artery (labels read from top: tunica externa, tunica media, tunica intima, smooth muscle, internal esastic membrane, vasa vasorum, external elastic membrane, nervi vasorum, endothelium, elastic fiber), and the top right panel shows the ultrastructure of a vein (labels read from top: tunica exerna, tunica media, tunica intima, vasa vasorum, smooth muscle, endothelium). The bottom panel shows a micrograph with the cross sections of an artery and a vein. [Return to Figure 13.2].
Figure 13.3 image description: The major arteries in the human body. Labels read (from top, clockwise) right common carotid, left common carotid, axillary, pulmonary trunk, descending aorta, diaphragm, renal, superior mesenteric, gonadal, inferior mesenteric, common iliac, internal iliac, deep femoral, femoral, descending genicular, doraslis pedis, plantar arch, fibular, anterior tibial, posterial tibial, popliteal, palmer arches, exernal iliac, ulnar, radial, brachial, celiac trunk, ascending aorta, aortic arch, brachiocephalic trunk, right subclavian, vertebral. [Return to Figure 13.3].
Figure 13.4 image description: The major veins in the human body. Labels read (from top, clockwise) internal jugular, brachiocephalic, superior vena cava, intercostal, inferior vena cava, gonadal, lumbar, right and left common iliac, external iliac, internal iliac, deep femoral, femoral, posterior tibial, anterior tibial, dorsal venous arch, plantar venous arch, fibular, small saphenous, popliteal, great saphenous, digital, palmar venous arches, ulnar, median antebrachial, medial cubital, hepatic, basilic, brachial, cephalic, axillary, subclavian, externa jugular. [Return to Figure 13.4].
Figure 13.5 image description: This diagram shows how oxygenated and deoxygenated blood flow through the major organs in the body. Pulmonary circulation involves the lungs, pulmonary artery and vein, vena cava, and aorta. Systemic circulation involves the upper body, hepatic vein, renal vein, aorta, liver, hepatic artery, hepatic portal vein, stomach, intestines, renal artery, kidneys, and lower body. [Return to Figure 13.5].
Figure 13.6 image description: The pulse points as shown on a woman's body. Labels read (from top) temporal artery, facial artery, common carotid artery, brachial artery, radial artery, femoral artery, popliteal artery, posterior tibial artery, dorsalis pedis artery. [Return to Figure 13.6].
Figure 13.7 image description: This figure shows three test tubes with a red and yellow liquid in them. The left panel shows normal blood, the center panel shows anemic blood and the right panel shows polycythemic blood. Labels indicate plasma (water, proteins, nutrients, hormones etc.), buffy coat (white blood cells, platelets), and hematocrit (red blood cells). [Return to Figure 13.7].
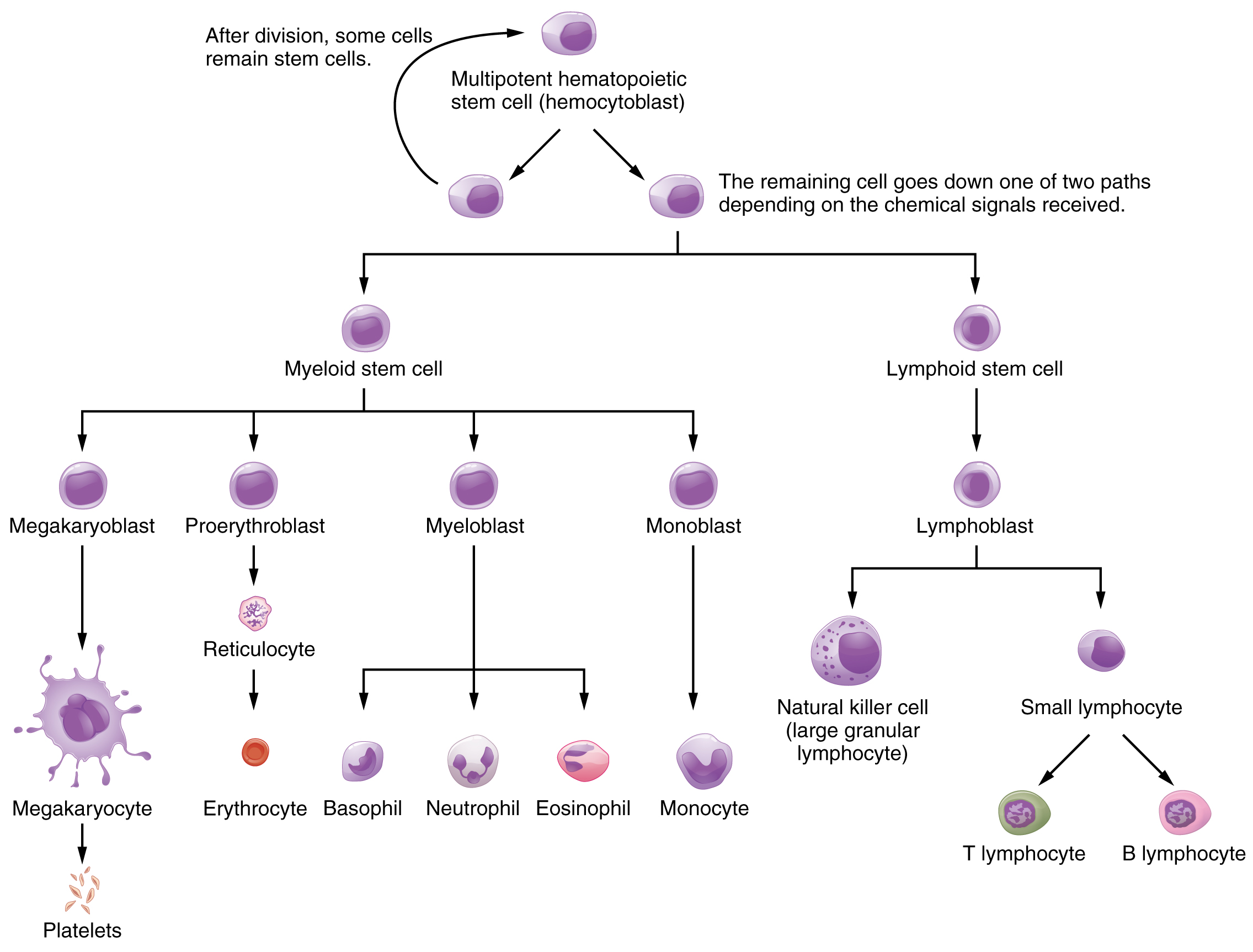
Figure 13.8 image description: This flowchart shows the pathways in which a multipotent hemotopoietic stem cell differentiates into the different cell types found in blood. From the top (multipotent hematopoietic stem cell can divide and some cells remain stem cells, while the remaining cell goes down one of two paths depending on the chemical signals received: myleoid stem cell or lymphoid stem cell. A myeloid stem cell then can become either a megakaryoblast (which then turns into a magakaryocyte, then becomes platelets), or it can become a proerythroblas (which then becomes a reticulocyte, then becoming an erythrocite), or it can become a myeloblast (which then becomes either a basophil, neutrophil, eosinophil), or it can become a monoblast (which then it becomes a monocyte). If the cell becomes a lymphoid stem cell, it then becomes a lymphoblas, which then becomes either a natural killer cell or a small lymphocyte ( either T or B lymphocyte). [Return to Figure 13.8].
Figure 13.11 image description: This figure shows how leukocytes respond to chemical signals from injured cells. The top panel shows chemical signals sent out by the injured cells (text labels read: 1) Leukocytes in the blood respond to chemical attractants released by pathogens and chemical signals from nearby injured cells). The middle panel shows leukocytes migrating to the injured cells (text labels read: 2)the leukocytes squeeze between the capillary wall as they follow the chemical signlas to where they are most concentrated (positive chemotaxis)). The bottom panel shows macrophages phagocytosing the pathogens (text label reads: 3) Within the damaged tissue, monocytes differentiate into macrophages that pgagocytize the pathogens.The eosinophils and neutrophils release chemicals that break apart pathogens. They are also capable of phagocytosis.). [Return to Figure 13.11].
Figure 13.12 image description: This figure details the steps in the clotting of blood. Each step is shown along with a detailed text box describing the steps on the left. On the right, a signaling pathway shows the different chemical signals involved in the clotting process. The steps described: 1. Injury: a blood vessel is severed. Blood and blood components (e.g. erythrocytes, white blood cells, etc.) are leaking out of the breaks. 2. Vascular spasm: the smooth muscle in the vessel wall contracts near the injury point reducing blood loss. 3. Platelet plug formation: platelets are activated by chemicals released from the injury site and by contact with underlying collagen. The platelets become spiked and stick to each other and the wound site. Initial platelets are activated by chemicals released from the injured cells and by contact with broken collagen. Bound platelets release chemicals that activate and attract other platelets. platelets move toward source of chemical signals and bind. Platelet plug grows in size. 4. Coagulation. In coagulation, fibrinogen is converted to fibrin (see part b), which forms a mesh that traps more platelets and erythrocytes, producing a clot. Part B Fibryn synthesis cascade: Intrinsic pathway (damaged vessel wall), Extrinsic pathway (trauma to extravascular cells), final common pathway (cross-linked fibrin clot). [Return to Figure 13.12].
Figure 13.14 image description: This figure shows an umbilical artery and vein passing through the placenta on the top left. The top right panel shows the first exposure to Rh+ antibodies in the mother. The bottom right panel shows the response when the second exposure in the form of another fetus takes place. Textboxes detail the steps in each process: First exposure birth of first Rh+ infant: 1. During birth, Rh+ fetal erythrocytes leak into maternal blood after breakage of the embryonic chorion, which normally isolates the fetal and maternal blood. 2) Maternal B cells are activated by the Rh antigen and produce large amounts of anti-Rh antibodies. Second exposure: Rh+ fetus: 3) Rh antibody titer in mother's blood is elevated after first exposure. 4) Rh antibodies are small enough to cross the embryonic chorion and attach the fetal erythrocites. [Return to Figure 13.14].
Figure 13.16 image description: The left panel (a) shows the cross-section of a normal and a narrowed artery. A normal artery has no plaque along the artery walls which means there is normal blood flow. In a narrow artery, plague forms on the arterial walls causing abnormal blood flow. The right panel (b) shows a micrograph of an artery with plaque in it. [Return to Figure 13.16].
Figure 13.18 image description: This photograph shows red blood cells of a person suffering from sickle cell anemia. Instead of being discoid shaped like healthy blood cells, sickle red blood cells are shaped like a sickle. [Return to Figure 13.18].
Unless otherwise indicated, this chapter contains material adapted from Anatomy and Physiology (on OpenStax), by Betts, et al. and is used under a a CC BY 4.0 international license. Download and access this book for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction.
