
1.5 Childhood trauma
WHAT IS TRAUMA?
Experts explain that trauma is not an event itself, but rather a response to a stressful experience in which a person’s ability to cope is dramatically undermined. More than 20 years ago, Lenore Terr (1992) defined childhood trauma as the impact of external forces that “[render] the young person temporarily helpless and [break] past ordinary coping and defensive operation. . . .” Terrasi and de Galarce (2017, p. 36) suggest that complex trauma is “the cumulative effect of traumatic experiences that are repeated or prolonged over time”.
Similarly, de Thierry (2017, p. 14) writes, “Trauma is an event or series of events such as abuse, maltreatment, neglect or tragedy that causes a profound experience of helplessness leading to terror”. As discussed earlier, the range of potentially traumatic events in childhood is quite broad, including not only physical threat and harm but also emotional maltreatment, neglect, abandonment, and devastating loss.
Every traumatic experience is different, and each child’s response depends on their coping skills and resources and on the context and circumstances in which the stressful event occurs. Whether a child develops a trauma reaction that increases in severity, becomes chronic, and is less responsive to intervention or has a reaction that is moderate, manageable, and time limited depends on several factors. These include the nature of the experience, the characteristics of the child, and the way the family, school, and community respond. For example, chronic or repetitive traumatic experiences, especially those perpetrated intentionally by a caregiver, are likely to result in a different set of symptoms than a single shocking traumatic event.
DETERMINANTS OF TRAUMA REACTIONS
Trauma results from an event, series of events, or set circumstances that is experienced by individual as physically emotionally harmful life threatening and has lasting adverse effects on the individual’s functioning mental, physical, social, emotional, spiritual wellbeing. The Substance Abuse and Mental Health Services Administration (SAMHSA) provide a useful ‘The Three E’ framework to understand how traumatic events impact on individuals (SAMHSA, 2013).
Events: The first ‘E’ of the framework refers to events – this is the circumstances surrounding the actual or extreme threat of physical or psychological harm (i.e., physical violence, natural disasters etc.) or severe, life threatening neglect for a child that imperils healthy development. These events and circumstances may occur as a single occurrence or repeatedly over time.
Experience: The individual’s experience of these events or circumstances helps to determine whether it circumstances helps to determine whether it experienced as traumatic for one individual and not for another (e.g., a child removed from an abusive home experiences this differently than their sibling; one refugee may experience fleeing one’s country differently from another refugee). How the individual labels, assigns meaning to, and is disrupted physically and psychologically by an event will contribute to whether or not it is experienced as traumatic. Traumatic events by their very nature set up a power differential where one entity (whether an individual, an event or a force of nature) has power over another. They elicit a profound question of “why me?” The individual’s experience of these events or circumstances is shaped in the context of this powerlessness and questioning.
Feelings of humiliation, guilt, shame, betrayal, or silencing often shape the experience of the event. When someone experiences physical or sexual abuse, it is often accompanied by a sense of humiliation, which can lead the person to feel as though they are bad or dirty, leading to a sense of self-blame, shame and guilt. In cases of war or natural disasters, those who survived the traumatic event may blame themselves for surviving when others did not. Abuse by a trusted caregiver frequently gives rise to feelings of betrayal, shattering a person’s trust and leaving them feeling alone. Often, abuse of children and domestic violence are accompanied by threats that lead to silencing and fear of reaching out for help. How the event is experienced may be linked to a range of factors, including the individual’s cultural beliefs (e.g., the subjugation of women and the experience of domestic violence), availability of social supports (e.g., whether isolated or embedded in a supportive family or community structure) or to the developmental stage of the individual (i.e., an individual may understand and experience events differently at age five, 15 or 50).
Effects: The long-lasting adverse effects of the event are a critical component to trauma. These effects may occur immediately or may have a delayed onset. The duration of the effects can be short to long term. In some situations, the individual may not recognise the connection between the traumatic events and the effects. Examples of adverse effects include an individual’s inability to cope with normal stressors, and strains of daily living; to trust and benefit from relationships; to manage cognitive processes – such as memory, attention, thinking, to regulate behaviour; or to control the expression of emotions. In addition to these visible effects, there may be an altering of one’s neurobiological make-up and ongoing health and wellbeing. Advances in neuroscience and an increased understanding of the interaction of neurobiological and environmental factors have documented the effects of such threatening events.
Traumatic effects, which may range from hyper-vigilance or a constant state of arousal, to numbing or avoidance, can eventually wear a person down, physically, mentally and emotionally. Survivors of trauma also highlight the impact of these events on spiritual beliefs and the capacity to make meaning of these experiences.
CHILD DEVELOPMENT AND TRAUMA
REACTIONS
The following points give an essential perspective for using the information about childhood trauma and its impact on development across specific age groups:
- Children, even at birth, are not ‘blank slates’ – they are born with a certain neurological make- up and temperament. As children get older, these individual differences become greater as they are affected by their experiences and environment. This is particularly the case where the child is born either drug dependent or with fetal alcohol syndrome.
- Even young babies differ in temperament e.g., activity level, amount and intensity of crying, ability to adapt to changes, general mood, etc.
- From birth on, children play an active role in their own development and impact on others around them.
- Culture, family, home and community play an important role in children’s development, as they impact on a child’s experiences and opportunities. Cultural groups are likely to have particular values, priorities and practices in child rearing that will influence children’s development and learning of particular skills and behaviours. The development of children from some cultural backgrounds will vary from traditional developmental norms, which usually reflect an Anglo-Western perspective.
- As children get older, it becomes increasingly difficult to list specific developmental milestones, as the achievement of many of these depends very much on the opportunities that the child has to practice them, and also, on the experiences available to the child. A child will not be able to ride a bicycle unless they have access to a bicycle.
- Development does not occur in a straight line or evenly. Development progresses in a sequential manner, although it is essential to note that while the path of development is somewhat predictable, there is variation in what is considered normal development. That is to say no two children develop in exactly the same way.
- The pace of development is more rapid in the early years than at any other time in life.
- Every area of development impacts on other areas. Developmental delays in one area will impact on the child’s ability to consolidate skills and progress through to the next developmental stage.
Most experts now agree that both nature and nurture interact to influence almost every significant aspect of a child’s development.
- General health affects development and behaviour. Minor illnesses will have short to medium term effects, while chronic health conditions can have long-term effects. Nutritional deficiencies will also have negative impacts on developmental progression. Specific characteristics and behaviours are indicative only. Many specific developmental characteristics should be seen as ‘flags’ of a child’s behaviour, which may need to be looked at more closely, if a child is not meeting them. Teachers and education staff should refer to relevant specialist assessment guides in undertaking further assessments of child and family.
The indicators of trauma listed in this guide should not become judgements about the particular child or family made in isolation from others who know the child and family well, or from other sources of information. However, they are a useful alert that a more thorough contextual assessment may be required.
There has been an explosion of knowledge in regard to the detrimental impact of neglect and child abuse trauma on the developing child, and particularly on the neurological development of infants. It is critical to have a good working knowledge of this growing evidence base so that we can be more helpful to families and child focused.
The following basic points are useful to keep in mind and to discuss with parents and young people:
- Children need stable, sensitive, loving, stimulating relationships and environments in order to reach their potential. They are particularly vulnerable to witnessing and experiencing violence, abuse and neglectful circumstances. Abuse and neglect at the hands of those who are meant to care is particularly distressing and harmful for infants, children and adolescents.
- Given that the infant’s primary drive is towards attachment to a parent or caregiver, not safety, they will accommodate to the parenting style they experience. They have no choice given their age and vulnerability, and in more chronic and extreme circumstances, they will show a complex trauma response. They can eventually make meaning of their circumstances by believing that the abuse is their fault and that they are inherently bad.
- Infants, children and adults will adapt to frightening and overwhelming circumstances by the body’s survival response, where the autonomic nervous system will become activated and switch on to the freeze/fight/flight response. Immediately the body is flooded with a biochemical response which includes adrenalin and cortisol, and the child feels agitated and hypervigilant. Infants may show a ‘frozen watchfulness’ and children and young people can dissociate and appear to be ‘zoned out’.
- Prolonged exposure to these circumstances can lead to ‘toxic stress’ for a child which changes the child’s brain development, sensitises the child to further stress, leads to heightened activity levels and affects future learning and concentration. Most importantly, it impairs the child’s ability to trust and relate to others. When children are traumatised, they find it very hard to regulate behaviour and soothe or calm themselves. They often attract the description of being ‘hyperactive’.
Babies are particularly attuned to their primary carer and will sense their fear and traumatic stress. This is particularly the case where family violence is present. They will become unsettled and therefore more demanding of an already overwhelmed parent. The first task of any service is to support the non-offending parent and to engage the family in safety.
- Traumatic memories are stored differently in the brain compared to everyday memories. They are encoded in vivid images and sensations and lack a verbal narrative and context. As they are unprocessed and more primitive, they are likely to flood the child or adult when triggers like smells, sights, sounds or internal or external reminders present at a later stage.
- These flashbacks can be affective, i.e., intense feelings, that are often unspeakable; or cognitive, vivid memories or parts of memories, which seem to be actually occurring. Alcohol and drug abuse are the classic and usually most destructive attempts to numb out the pain and avoid these distressing and intrusive experiences.
- Children are particularly vulnerable to flashbacks at quiet times or at bedtimes and will often avoid both, by acting out at school and bedtimes. They can experience severe sleep disruption and intrusive nightmares which add to their ‘dysregulated’ behaviour, and limits their capacity at school the next day. Adolescents will often stay up all night to avoid the nightmares and sleep in the safety of the daylight.
Now that we know about the impact of the risk factors and of childhood trauma we can begin thinking functionally about the needs of these students and begin by considering the factors depicted in the triangle, heart and speech bubble shapes in the figure below.
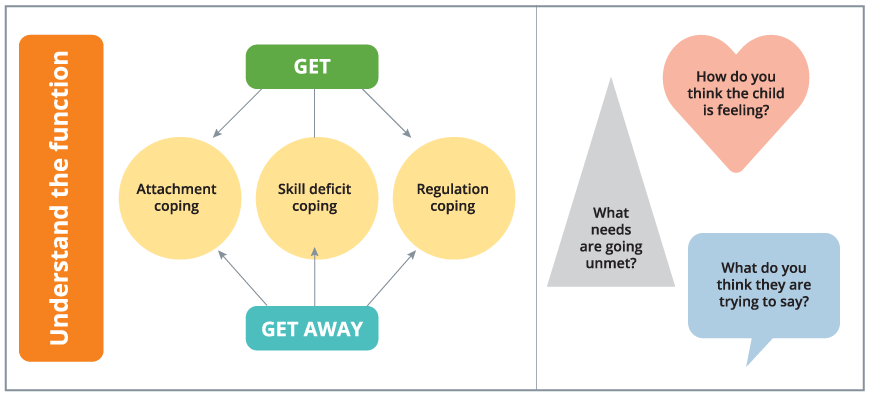
The triangle represents the pyramid of needs (see Snowman et al., 2009 for Maslow’s hierarchy of needs) starting with physiological needs, such as adequate food, hydration, clothing and physical health care. Examples of how this can be supported in the school environment include rest times, snack times built into learning time, water bottles on desks and available at all times throughout the day, and breakfast clubs.
The heart represents the feelings of grief linked to the losses in the child’s life that may impact their academic and social functioning at school. These losses may include the death of loved ones, separation from family and friends, and traumatic grief linked to experiences of abuse. Understanding these losses and their impact on the student can inform our expectations of the student’s functioning, the management of the classroom and school environment to minimise triggers and the support for the student to build trusting relationships that can help them with these complex and painful feelings.
The speech bubble shape represents the student’s behaviour as communicating unmet needs and unprocessed feelings. The deprivation and abuse experienced by these children often leaves them with deficits in their skills to seek out appropriate support. Due to this, the child’s misbehaviour may come across as deliberately defiant and oppositional, when in fact, it may the result of their inability to appropriately communicate the challenges that they are facing. It is then, the job of the educators to understand the context of the child – both in and out of the school environment – to interpret the function and meaning of the misbehaviours and disengagement.
The next section will look in depth at how we can use our knowledge of childhood trauma in adapting our pedagogical practices.
References
de Thierry, B. (2017). The simple guide to child trauma. What it is and how to help. London, UK: Jessica Kingsley.
SAMHSA Trauma and Justice Strategic Initiative (2013). SAMHSA’s concept of trauma and guidance for a trauma-informed approach. Retrieved from https://store.samhsa.gov/system/files/sma14-4884.pdf.
Snowman, J., Dobozy, E., Scevak, J., Bryer, F., & Bartlett, B. (2009). Psychology applied to teaching. Milton: Australia: John Wiley & Sons.
Terrasi, S., & de Galarce, P. C. (2017). Trauma and learning in America’s classrooms. Phi Delta Kappan, 98(6), 35-41.
